
Victims of Psychiatry in Malta: Exposing a System of Abuse
In psychiatry, it is not the abuser who is held accountable, but rather the person who dares to speak out against the abuse. One can expect no apology to a patient; instead, they are retaliated against by all means for putting these 'cosy' jobs and this fake profession at risk.
“Are you hearing voices? Having bad thoughts? Are you sleeping at night? Do you think someone is against you? Are you eating…?”
The same hollow questions, repeated endlessly — like a script they recite without ever listening. Every encounter with a psychiatrist feels like being pushed through a machine that doesn’t care who you are or what you feel.
They strip away the few freedoms you have left, locking you behind the ward’s doors day and night, cutting you off from the outside world with communication bans. They push more pills, more injections — layers of sedation that swallow your personality until you barely recognize yourself. And the side effects… shaking hands, stiff limbs, parkinsonism, the loss of intimacy, the feeling that your own body is turning against you.
Once they are satisfied with how much they’ve diminished you, they smile smugly and tauntingly say ..., “You look much better now, so calm” — gratifying themselves as if they were spot-on in addressing your supposed symptoms. But if not, or if you dare confront them...
Then they stand there and claim you look “excited,” “agitated,” “aggressive,” “disturbed” — as if they’re waiting for one wrong expression, one trembling word, just to justify another dose, another experiment.
It’s like they wound you and then pretend to be the ones offering a cure, treating the very symptoms they created in the first place. A cycle of harm disguised as help, leaving you feeling powerless, unheard, and trapped.


From Wikipedia's article Controversies about psychiatry: As long as psychiatry has existed, it has been subject to controversy. Psychiatric medications are sometimes regarded as ultimately more damaging than helpful to patients. Psychiatry is sometimes seen as a benign medical practice, but at times it is viewed by some as a coercive instrument of oppression. It is often criticized for involving an unequal power relationship between doctor and patient, and for relying on a subjective diagnostic process that leaves much room for opinion and interpretation. In 2013, psychiatrist Allen Frances stated that "psychiatric diagnosis still relies exclusively on fallible subjective judgments rather than objective biological tests."
This statement by Allen Frances — a psychiatrist himself who had the audacity to criticize his own profession — gives a clue to the abuses behind psychiatry. Despite relying exclusively on "fallible subjective judgments," psychiatrists, without any scientific basis (such as urine tests, blood tests, or brain scans), diagnose people as mentally ill and prescribe unnecessary medications with terrible side effects (see article: 12 Shocking Facts About the Dangers of Psychiatric Drugs). They do so without conscience, showing little scruple or principle, so long as it enriches them at the expense of their patients. To illustrate: imagine a doctor who is unsure whether you actually have AIDS (assuming it cannot be detected through blood tests or any scientific method), but administers AIDS treatment anyway — or worse, deliberately labels you with the illness to discredit and character-assassinate you, as happened to me in my first court case, where I ended up being labeled as mentally ill just to save Magistrate Carol Peralta’s career.

But if you really want to know how FAKE psychiatry is, don’t bother asking psychiatrists — they’re too busy protecting their own interests and covering up the truth about their bogus profession. ASK THEIR VICTIMS. Here are some of patients I met during my time in Male Ward 3A at Mount Carmel Hospital — true victims of that FAKE branch of medicine they dare to call psychiatry.
Male Ward 3A victims I witnessed men being ruined by psychiatric medication — lives steadily dismantled under the weight of drugs they could not refuse.

In the image above, next to each patient’s name is the injection they were prescribed — the invasive treatment they underwent. Three patients marked in green were alcoholics (one is shown in more detail here) and were diagnosed as schizophrenic, receiving injections of Haldol and Fluanxol. Like in my case, no scientific tests — blood, urine, or brain scans — were performed; psychiatry relies on presumptions, not facts.
These injections did not stop their alcoholism. Addiction cannot be cured by drugs alone — willpower is essential. Psychiatry often escalates dosages until patients are sedated and disabled, solving “problems” in a cruel, artificial way.
The patient marked in orange was over 80 in 2018. The Fluanxol leaflet warns: “You are more at risk for abnormal heart rhythm if you are older than 65.” The patient in red was almost 74, and the Modecate leaflet states: “Check with your doctor if you are elderly (65+) or in poor health.”
The patient marked in blue, in his 30s in 2018, received Fluanxol 400mg every two weeks. The leaflet recommends such high doses only during acute relapse, with a gradual reduction to 20–200mg for maintenance. Even when I was reduced to 20mg every 4 weeks, it made life unbearable — imagine 400mg fortnightly, forty times higher.
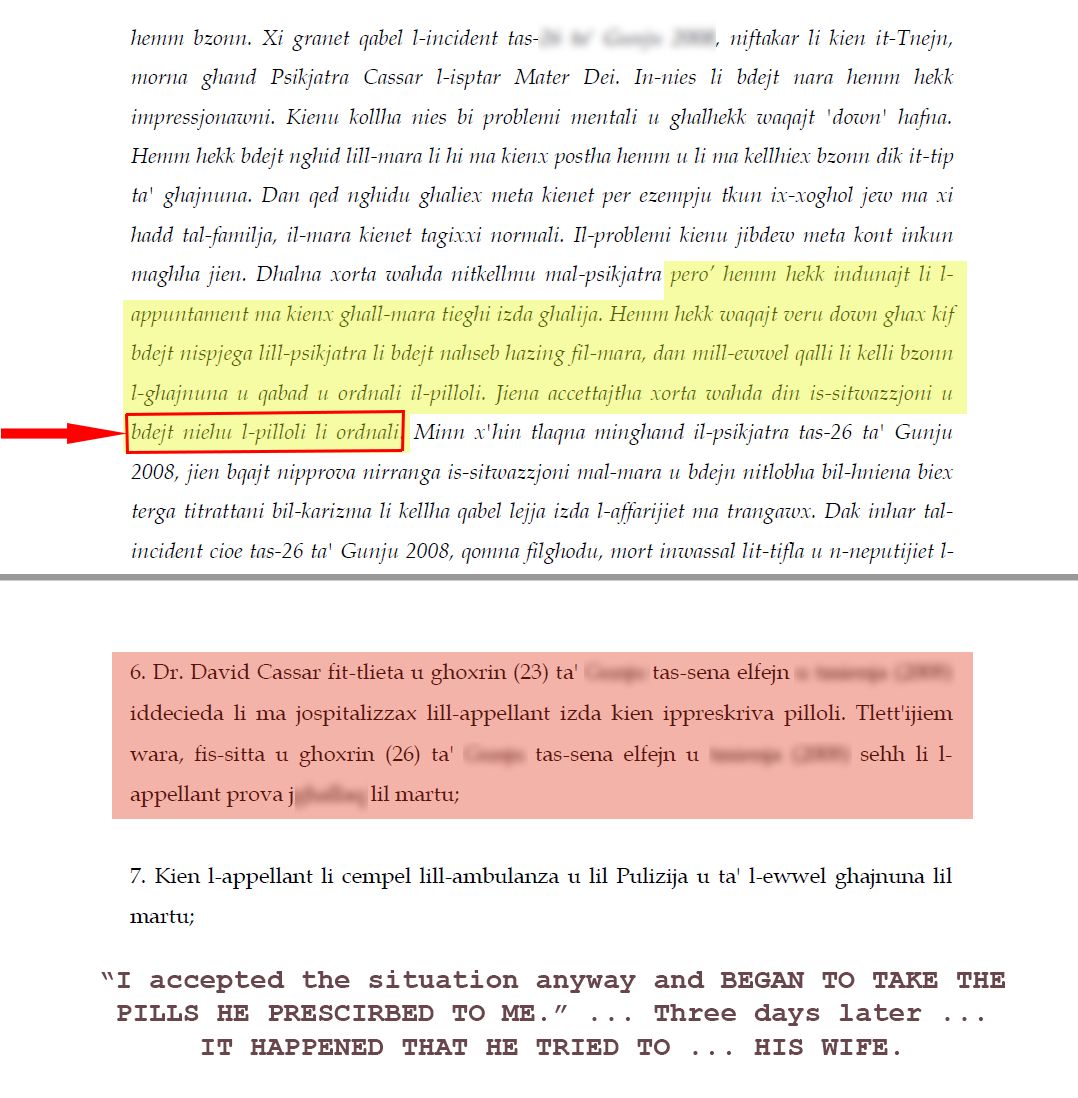
The patient in pink had a full-time job in 2008. In court, he claimed mental issues during a crime — likely as an excuse to reduce responsibility — something almost anyone instinctively does when faced with psychiatric assessments, which are most often fake. Psychiatric opinions conflicted: three doctors wanted him held accountable, while one, believing he knew better, opted to excuse him as mentally insane to save him the job, thus ensuring he remained available for further experimentation with psychiatric drugs.
On that 7 October 2018 (a Sunday, possibly the day he was to receive the next injection), this patient, still employed full-time and with no actual workplace problems (the “problems” being fabricated psychiatric illusions), had his Risperdal Consta dosage increased by 25%, from 50mg to 62.5mg every fortnight. Most likely, he did not exhibit any symptoms warranting such an increase. This adjustment was probably linked to his three-month prison sentence, which was under appeal. His consultant psychiatrist, David Cassar, may have used the increased dosage to present a “favorable” image in court, resulting in the sentence being reduced to a three-year suspended sentence in March 2019. About a month before, Cassar had testified that the patient was on the “highest dose of Risperdal Consta.” See also this link from the Court of Appeal judgment regarding the same patient, explained further
{kind=link}
Once again, psychiatry shows its lack of scientific grounding: to avoid prison and safeguard his job, this patient was forced to endure experiments on his health at a higher dose. Consulting psychiatry in court is like consulting a high priest or fortune teller to predict future wrongdoing — only worse, because it is effectively assessing whether the person has been sedated, drugged, or disabled enough under the guise of psychiatric treatment.

Not on the above list is a certain undocumented immigrant from Somalia who, like others, may pretend to be depressed or to hear voices in order to claim social benefits at taxpayers’ expense. He may even qualify as a “social case” and be placed in a community home, where he is forced to take harmful injections. That doesn’t seem to bother him, since he freely spends his days smoking (with money from social benefits) and adding three spoonfuls of sugar to every coffee.
People like him are especially vulnerable to being maliciously diagnosed with schizophrenia, often with the convenient excuse of “immigration-related social adversity and racial discrimination.” One day, while at the Mount Carmel Hospital precincts, he allegedly exposed his genitals to a passing woman. Certainly not something commendable — but what followed was even worse. The woman reported him — probably to MW3A staff or the police, who then referred him to the ward. In response, the psychiatrist increased his injection of Risperdal Consta to 75 mg every fortnight. Among other things, this drug can cause impotence, which made the punishment all the more obvious. They were prescribing it not for healing, but specifically for its dreadful side effects. In this case, the justification was that it would prevent him from repeating the same behavior. In reality, they effectively sterilized him — solving the “problem” by destroying his body. Like cutting off someone’s hands to stop them from stealing.
For women, the pattern is similar. Instead of children being “prevented” by similarly harsh injections, sterilization can also mean forcing an intrauterine device (IUD) into her uterus. And yes, the leaflet itself admits: “Your periods can be heavier, longer, or more painful in the first 3 to 6 months after an IUD is put in.”
Back to the Somali man: he also began vomiting frequently — another side effect of Risperidone. But the staff never cared. They simply let him vomit again and again, without reporting it. Let’s be generous and say they didn’t do it out of pure negligence, but because side effects like these are so common with psychiatric drugs. Maybe they wanted to spare the patients the excuse of being “treated” with yet more pills — since that would mean extra work for the nurses.

And if the patient dares to complain about side effects — especially ones listed in the official leaflet, which clearly says to inform the doctor — the response is vile. They twist it to claim it cannot be the same symptom, because manufacturers only list such effects for insurance reasons. If the suffering is undeniable, and they see with their own eyes the damage caused, they still won’t blame the drug. Instead, you risk being overdosed with other pills to “treat” the new side effects, or subjected to even more invasive interventions like Kemadrin injections. Worst of all, they may accuse you of faking the symptom simply because you read about it in the leaflet.
That’s exactly what they did with me when they had to prescribe me those additional Artaine pills to combat the frightening side effects of Fluanxol / Depixol. You need immense mental strength not to collapse in despair when you are treated so vilely and mocked so openly.

For sure, no one hears your cries. You just have to keep suffering in silence, learn to live with the side effects, and try not to predict the state you will be reduced to in the long run as you grow older and weaker.
There are also cases where, I presume, one cannot find a place in some government-run old people's homes, like St. Vincent de Paule, to simply lock away their parents. So they take a chance and go to a private, often fake, psychiatrist, inventing some excuse for them to inflate even more in order to commit their parents instead to Mount Carmel Hospital. Labeling someone as mentally ill is so easy that you don’t even need to be a psychiatrist to do it—though, of course, psychiatrists will gladly do the rest.
For example, there was an old man in his 80s (b. 14.2.1934?) who, for enjoying spending some of his hard-earned savings on a car, ended up locked away by three of his five children. They had already considered that money as being theirs and used the excuse that he was wasting it. He had made the mistake of transferring his property during his lifetime rather than in a testament, which made him a “burden” in their eyes in order to gain access to whatever else he owned in cash. As the Latin proverb goes: Male secum agit aeger, medicum qui heredem facit — a sick man acts badly when he makes a doctor his heir.
Another case occurred at MW3A around 2018, where an old man was locked away, likely due to an excuse of depression invented by his daughter to get rid of him. (In this link, his niece, not his daughter, is listed as the contact person.) The daughter had signed all necessary papers for him to be treated and drugged at the discretion of psychiatrist David Cassar. Cassar, undoubtedly seeing another victim, began malicious experiments on him, including electroconvulsive therapy (ECT). This old man was given about 24 electrically induced seizures — roughly four times the normal amount, as typical ECT is administered two to three times a week for six to twelve sessions.

On the 21st session, the old man suffered a heart attack, one of the well-known risks of ECT, especially for the elderly (see article: ECT depression therapy should be suspended, study suggests). Cassar had nearly succeeded in killing him, while the daughter showed virtually no concern, having lost interest in her father the moment she had him committed and signed the papers allowing Cassar to proceed. Fortunately, the niece took care of him and had protested from the start, insisting he was not mentally ill (He seemed like an ordinary elderly man, with whom I had the pleasure of discussing old Maltese currency used under the British, and how people referred to it using terms from the Knights’ era — for example, the ‘xelin’ and ‘8 soldi,’ or ‘20 soldi’ was called a ‘skud,’ and so on). Only because of her persistence did Cassar abandon further ECT treatments.

From reliable sources, I heard that Cassar had to make a U-turn, declaring that the old man was fit to leave the hospital if he wished and live independently — likely to free up that space for the next victim on whom he could more freely and at leisure experiment. The man ultimately passed away at the beginning of November 2020.
First, they vindictively suffocated him, only to resuscitate him to cover their tracks. Acting as saviors by reviving him neither excuses nor exempts them from the fact that they were his executioners just minutes prior.
Also, at MW3A, a patient in his twenties — who most likely suffered from schizophrenia (he was reported to hear voices, etc.) — sometimes became somewhat violent, breaking window glass and engaging in similar behaviors. Cassar appeared to have overdosed him with multiple medications in an attempt to sedate him (I once heard a nurse say, “I had enough preparing his pills” / “Xbajt naghmillu l-pirmli”). He was prescribed numerous medications and subjected to many ECTs, yet he continued to hear voices — if anything, they increased — and it seems unlikely he will reach 40 without being completely disabled by the side effects of all those drugs.
On Monday, July 17, 2017, at approximately 10:00 a.m., he became agitated and violent toward the staff, escalating after one nursing aide further provoked him. Due to his physically imposing stature, three or four staff members surrounded him. One nurse restrained him by the neck while the group forced him to the floor. While pinned, he suffocated and was unable to breathe, due to either the collective weight of the staff piling on top of him or the pressure exerted on his neck.
When the staff eventually turned him face up and realized he was not breathing, their immediate reaction indicated panic that their use of excessive force had already caused his death. Another nurse involved had such charisma in dealing with patients that, on 4-Apr-18, he threw my food away when I tried to expose staff abuses (see further details below).Yet he was the one who initiated CPR, and managed to resuscitate him again. His family was contacted (his mother arrived), along with his consultant psychiatrist, David Cassar (fortunately it was a Monday; on Fridays he used to be present, but on other days he was rarely around despite supposedly holding a full-time position), and an ambulance. He was transported to Mater Dei Hospital, where he remained for several days under observation.
The fact that such a youth was rushed to the emergency department yet showed no symptoms indicating fits or a heart attack should have been an eye-opener that something serious had occurred. Yet no one ever bothered to carry out an investigation to see what had actually happened, perhaps to avoid creating issues with colleagues at another hospital, staying silent even about the adverse effects from the overdosing and multiple medications administered by David Cassar himself.
The unavoidable question is this: even if resuscitation succeeded, does the act of reviving him in any way negate the reality that, based on the events observed, the force used had already pushed him to the threshold of death? One cannot simply disregard the fact that he had to be brought back to life only minutes after being restrained. The incident stands as a stark indication that the level of force applied was not merely excessive but — by any reasonable interpretation — force that had already proved fatal until reversed.
Two patients on so-called “psychiatric cure,” whose crimes were considered atrocious, both died in their 50s. This is what passes for care.
Another case worth mentioning is that of a man named SM, nicknamed Kalanc, whom I first got to know in 2002, when Psychiatrist David Cassar and Magistrate Carol Peralta abusively had me kidnapped and locked up in what was then Male Ward 10 at Mount Carmel Hospital. I met him again during my second court case, in the 100 days I spent in the Forensic Ward until my sentence was handed down on 26 June 2014.
He had been sentenced by the court to life imprisonment, and what struck me most upon seeing him again was how badly his health had deteriorated between 2002 and 2014 — in just 12 years. I later heard that he died in 2019, at only about 54 years of age, from heart complications.
I am totally convinced that his death was caused by the side effects of the drugs he was overdosed with. He did not have heart problems before being locked up in this hospital; they were probably not genetic either, and certainly not the result of heavy smoking. His only source of income was the small benefits he received while locked in prison/hospital, which limited how much he could spend on cigarettes, and of course he ate the very “healthy” food provided by the hospital.
Most likely, they experimented even further on him after his beloved mother passed away. She used to visit him every single day and bring him food (“kienet tiġi tarani kuljum, ustja” / “she used to come to see me every day”). When he was locked in Male Ward 10, this meant that his mother spent at least two hours travelling by bus from Żejtun to the hospital in Ħ’Attard and back home, just to see her son and exchange a few words with him during the mere 15 minutes allowed.
After her death, he ended up almost forgotten and abandoned by his remaining relatives. While we were in the Forensic Ward, he told me that he had another brother or two who very rarely came to see him (“għandi ħija ieħor imma ilu ma jiġi jarani” / “I have another brother, but it has been a long time since he last came to see me”).
Of course, the crimes he committed are not something to be commended, whether they were done while drunk or under the influence of drugs (psychiatric drugs?). As said in Psychiatric drugs? - violence and suicide booklet, worth noting the man mentioned earlier whose sentence was reduced on appeal had been prescribed pills by Psychiatrist David Cassar just three days before he committed what was most probably his only crime.
Yet everything is perfectly fine for the psychiatrist(s), comfortably paid from public coffers and fully in control of their senses, to have most probably and blatantly killed this man, while making his life miserable through the side effects of the drugs they prescribed.
But if you think this was just an isolated incident, you are mistaken. During my stay at Forensic in 2014, I also came to know a man named Harrington, who, during the roughly 25 years he was locked in this hospital/prison, ended up completely disabled — unable to speak, shaking with tremors, and suffering from other severe conditions.
In some cases, they issue a Treatment Order (TO), meaning that the Court or another authority gives consent to a psychiatrist to prescribe whatever treatment they see fit, whether the patient agrees or not. In Malta, a Treatment Order is literally capital punishment under a different, more pleasing name, with the “executioner” renamed as “psychiatrist.” In fact, it is even more diabolical: the culprit is made to pay for his crimes by being destroyed slowly through the side effects of psychiatric medication over a prolonged period, so as not to raise suspicion, making it appear as though his health had been deteriorating naturally — when in reality the deterioration began with the psychiatric medication itself.
To put it simply, in Malta, whenever the Court wants to impose capital punishment on someone — sometimes on the suggestion of the corrupt police themselves, given the vile way they frame up the accused — it appoints the usual psychiatrist to fabricate a report claiming that the person is paranoid, psychopathic, schizophrenic, and so on. Using this excuse, the person is placed on a Treatment Order (that is, effectively sentenced to death), which the psychiatrist then “executes” by slowly destroying the individual through the diabolical side effects of psychiatric drugs. Meanwhile, the victim serves as a guinea pig for drug experimentation, paying society with his life and health for his alleged crimes (examples from our time include this one put on Modecate and another one put on Risperidone).
They claimed that Harrington suffered from Huntington’s disease, dementia, Parkinsonism, or something similar — once again, a perfect excuse to experiment with drugs on him. I am totally convinced that he was reduced to that state within just a few years, with his decline accelerated by the side effects of the psychiatric drugs he was prescribed and overdosed with. He died later that same year, in 2014. If he was 43 years old in 2000, then in 2014 he was only 57 — another likely intentionally induced and dreadful death in this fake hospital, at the hands of psychiatrists.
Of course, reporting such things is useless. You will always find many people ready to invent ridiculous excuses to cover these crimes, refuse to respond, or even turn against you. People in high positions in Malta protect each other’s corrupt practices, and they will make your life hell if you dare to challenge any one of them — like a kind of Masonic organization.
Once again, everyone condemned Harrington for allegedly burning his victim alive, yet for the Court to authorize psychiatrists to burn his life away in such a dreadful manner goes completely unnoticed, if not outright justified. Our local media, too, finds nothing suspicious or worthy of investigation in such cases.
But let us analyze the similarities. Impressively, in both cases:
- Mangion and Harrington died in their 50s, despite living on a supposedly healthy diet in that hospital.
- Both were under the influence of psychiatric medication — SM for more years, which probably contributed to him dying younger.
- Both ended up in the same ward (forensic).
- Both had committed crimes that instigated enormous hatred against them, with many Pharisees (in a typical country where the more corrupt you are, the more you are adored — so expect to find many) wanting them killed in the most atrocious and savage ways, which served as a further incentive for psychiatrists.
- Both were involuntarily committed and hospitalized.
- Both were detained under a court order, which meant they could not refuse — let alone object to — the psychiatric drugs imposed and enforced on them, treating them like guinea pigs.
I have just given you six hints, six facts. Yet many people are so blinded that they still find nothing wrong with psychiatry. On the other hand, a psychiatrist needs only to invent a single lie — maliciously labeling you as mentally ill — for everyone to believe him, as if his words came from a sacred textbook.
Both cases share so many similarities that it is blatantly obvious their premature deaths were certainly not a coincidence.
Once again, if you are so blinded that you ignore these atrocities and facts, and believe I am deliberately exaggerating, then visit the webpage containing Malta’s Mental Health Act Schedules. See for yourself the near-total freedom psychiatrists are granted to abuse, experiment on, and silence patients — particularly the diabolical Schedule 14, Part 2 listed at the end (another copy provided here).
The Schedule states that “consent is in writing and signed by the person.” Let us charitably assume this deliberate ambiguity means the patient, while still in control of his senses and before being drugged — not some “other person,” such as a relative or so-called “responsible carer” with a vested interest in removing him. What this “consent” actually means in Malta is addressed further below, based on my own experience.
Schedule 14 concerns an “Application for Invasive or Irreversible Treatment.” Invasive treatment primarily refers to forced injections used to administer psychiatric drugs (as in my own case and in those shown further above). Irreversible treatment is even more disturbing, defined as treatment that has “unfavourable irreversible physical or psychological consequences.”
This has nothing to do with irreversible illness such as Alzheimer’s disease. Rather, it echoes discredited practices such as lobotomy — a procedure introduced in the late 1930s that quickly became a byword for medical barbarism, a textbook example of the trampling of patients’ rights, and is now widely regarded as one of the greatest atrocities in modern medicine — particularly psychiatry.
Such practices directly violate United Nations mental health human rights principles, specifically Clause 11(14): “Psychosurgery and other intrusive and irreversible treatments shall never be carried out on an involuntary patient.”
Yet in Malta, human rights appear reserved for the elite. All it takes is a malicious psychiatric label to be reduced to a guinea pig — another SM or Harrington in the making — waiting for the “box” to collect what remains of you: “minn hawn fil-kaxxa joħorġuk.”

Regarding the injection of Kemadrin listed next to some patients’ names in the image further above, it appears to be given in addition to treat symptoms of Parkinson’s disease or involuntary movements caused by the side effects of certain psychiatric drugs. This clearly shows how dangerous some psychiatric medications can be — they can even make you sick with conditions such as drug-induced parkinsonism. It’s remarkable (and troubling) that in psychiatry practitioners think that causing one set of symptoms will somehow cure another. It’s like taking a shoe to a cobbler for a tiny hole and ending up with an awful patch that ruins the shoe entirely — leaving you with nothing but wasted money and a broken shoe. In the case of psychiatry, the cost is your health and your life.
This is a YouTube video worth watching titled: “Psychiatry gave me Diabetes, Heart Disease, and Gynecomastia” (Tom’s Story)
 This is the Mosta Bridge after a fence was installed in 2016, allegedly to prevent suicides. Let’s be honest: if someone is in such despair that they are considering taking their own life, a fence will not stop them. They can bring a ladder or choose another site. By that logic, we should fence every building taller than one storey.
And ask yourself — does staring at a cage help anyone? Or is it better to see what little beauty remains of what was once a sacred, open valley?
This is the Mosta Bridge after a fence was installed in 2016, allegedly to prevent suicides. Let’s be honest: if someone is in such despair that they are considering taking their own life, a fence will not stop them. They can bring a ladder or choose another site. By that logic, we should fence every building taller than one storey.
And ask yourself — does staring at a cage help anyone? Or is it better to see what little beauty remains of what was once a sacred, open valley?Now that the view has been blocked, let the fence at least serve a purpose. Let it stand as a symbol of psychiatry itself: a web you cannot escape, a cage disguised as care, where others decide what is “good for you.” Another monument to cruelty hiding behind concern.
According to reporting, the decision was pushed by a psychiatrist: Mark Xuereb, a familiar face on Xarabank / The Bus, where he used to regularly dispense shallow platitudes. He formerly worked with the “Crisis Intervention” unit. Notably, despite early attempts to suppress his identity, he was probably the one arraigned in court on 13 May 2024 on stalking charges — allegedly a long-standing pattern — after even a commission failed to lift the ban on publishing his name.
There are also troubling first-hand accounts. One patient, BC, described how Xuereb advised his relatives to meet him privately, charged them around €250, and did nothing. When confronted later, Xuereb snapped: “Gejt theddidni?” (“You came to threaten me?”). His name has also surfaced in benefit-fraud cases, where certificates signed by him were used to secure approvals.
For Xuereb — and for psychiatry more broadly — the alternative to suicide prevention seems to be “managing your condition” with pills and injections: dependency, emotional flattening, and coercive medication with severe side effects. Refuse, and there is always a “Treatment Order,” supposedly “for your own safety.” The system stays profitable; the patient pays the price.
This stands in stark contrast to personal autonomy. Who am I to decide what you do with your life? Yet psychiatry claims that authority. In this system, the patient owns nothing — not even their own file, stamped with the chilling words: “NOT TO BE HANDLED BY THE PATIENT.”
The idea that you're in 'good hands' with a psychiatrist is a fallacy. Why waste money and health on 'professionally fake' cures? If a patient stops hearing voices but is left physically broken by psychiatric drugs, is that really a 'cure'? It’s a vicious cycle: treating one condition only to create another, like Parkinsonism, and then drugging the patient further to manage the new symptoms.
I knew of a patient in his 40s at Mount Carmel Hospital who, after years of psychiatric drugging, ended up obese, diabetic, and suffering from sleep apnea. Despite having a medical aid card, he had to pay out of pocket for a CPAP machine just to breathe at night. Of course, that device then caused dry mouth and air swallowing. Psychiatrists claim to cure one disease, but they only replace it with a multitude of others rather than addressing the source of the problem: their venomous pills and injections.
What is the purpose of "saving" someone from suicide, only to use them as a guinea pig? They are drugged, reduced to a disabled state, and killed slowly over time with the "fake medicine" of psychiatry. The goal isn’t to save a life, but to provide psychiatrists with another opportunity to line their pockets and feast on another victim.
Furthermore, committing suicide does not inherently imply mental illness—consider historical figures like Mark Antony and Cleopatra. In psychiatry, however, a difficult life period is exploited as an excuse to drug a person into a state of permanent dependency.
For instance, at Mount Carmel (MW3A), I knew a man named VG from Fgura. He was a skilled welder who had earned his position at the Malta Shipbuilding through merit — "kont dhalt bl-ezamijiet mhux bil-fottamenti" — rather than through connections. One day, perhaps due to depression, he attempted suicide by swallowing pills. He survived, but complications required the amputation of his thumb. Afterward, he was locked in the hospital by Psychiatrist David Cassar for six months.
Given he was likely already on psychiatric medication at the time of his attempt, it’s possible the attempt itself was a side effect. He died around July 22, 2016, likely still in his 50s. He was "saved" from suicide only to meet an early death, arguably caused by the very medications he was forced to take.
Suicide is more common among psychiatric patients because when a person is stripped of their dignity and destroyed by diabolic pills and injections, they may see suicide as the only way to escape the torture: the ultimate side effect of the side effect.
What is even more vile is that the nurses and staff are well aware of the damage psychiatric drugs inflict on patients, yet they simply do not care; it clearly does not weigh on their consciences. Why was it necessary for me — already in a disadvantaged position and discredited as a “mental patient” — to document these abuses? When those who work in this field, with hands-on experience of countless cases, remain completely silent.
Compare this to a teacher who remains silent while a headmaster blatantly and repeatedly abuses students. Could that teacher ever be excused or held unaccountable? Failure to report abuse makes you complicit. Instead, these staff members prioritize being the psychiatrists’ lackeys, choosing friendship with those in authority over professional integrity, all at the expense of the vulnerable patients in their trust. Their priority is simply that the payslip arrives at the end of the month — “l-aqwa li fl-ahhar tax-xahar tidholli l-paga” — and that they eventually get rid of another patient: “ahjar ghax xi darba nehilsu minn iehor.”
They seem to enjoy their roles in these crimes, acting as accomplices through their silence and by administering these "diabolic" treatments. If the psychiatrist is the magistrate who signs the order without a scientific basis, the nurses are the executioners who carry out the abuse with their own hands.
When I once tried to refuse medication after being destroyed by its side effects, the staff did not help me report the damage to my health. Instead, they instantly reported me to Psychiatrist David Cassar. They ignored the fact that I was being held in the hospital based on a completely wrong conclusion in a court report. Cassar even returned a letter I sent him on October 9, 2016, which was meant for my file. Though the staff had 24-hour access to my records, they never alerted the police. I eventually managed to retrieve the original letter — complete with fingerprints from Cassar and the MW3A staff — by asking a nurse to photocopy it at the SNO's office and keeping the original for myself.

If mine were an isolated case, one might instinctively suspect that the fault lies with me — perhaps that I am merely exaggerating. However, after outlining so many dreadful cases of victims of psychiatry, one must be either an imbecile blinded to the obvious, or a person with a malicious, vested interest in covering up these abuses through silence.
If you are still not convinced of the widespread abuse within the system, consider the following patient. He felt he had no choice but to hire a lawyer at his own expense: a certain Dr. Rachel L. Montebello. Dr. Montebello now holds the position of a Judge, having been promoted to that role from Magistrate as recently as 2018.


The following is a translation of the final three paragraphs from the first image; text in brackets indicates my own clarifying additions.
The complaint of my client concerns the fact that he was prescribed 'Modecate' many years ago as part of his hospital treatment. However, the dosage he has been receiving lately is excessive, to the point that Mr. [Name] is suffering from side effects that make his life far more miserable than his circumstances already dictate. Effectively, my client was being administered 150mg of Modecate every fortnight—a dosage which, according to general medical guidelines, is excessive. In fact, the standard medium dosage is in the 25mg range, with 100mg typically being the maximum.
The side effects Mr. [Name] is experiencing cause him great daily inconvenience and profound embarrassment. He frequently complains of dizziness, extreme fatigue, lethargy (lack of energy), and hypertension, as well as incontinence (lack of voluntary control over urination or defecation), which is deeply humiliating for him. Furthermore, he is unable to read for extended periods, which is a significant loss for him in these circumstances.
Following several consultations with his psychiatrist (likely initiated by the lawyer after the patient’s own complaints were ignored), the Modecate dose was lowered over recent months — first to 125mg every fortnight, and currently to 112.5mg. Nevertheless, the aforementioned side effects have not subsided despite the reduction, even though his condition remains satisfactorily under control at this lower dose.
Analysis: Note how this patient, GM, was originally administered Modecate at 150mg — the same dose given to the elderly man highlighted in red in the first image above. His psychiatrist is, once again, David Cassar. As this case confirms, Cassar appears to have long made the experimentation on patients a sadistic pastime. This letter mentions the dose was lowered to 125mg and then 112.5mg, which demonstrates either Cassar’s incompetence in prescribing dosages haphazardly or, more likely, that he was experimenting with the effects of an overdose.
The same patient recounted how he was once prescribed a pill which he refused to take. As a result, he was locked in the ward and his privileges were revoked. They claim treatment is given with 'consent,' but in reality, it is forced upon you. You are voiceless and stripped of rights the moment you are labeled 'mental.'
Once he was coerced into taking the drug, he suffered a seizure so severe he required emergency hospitalization. This illustrates just how dangerous these psychiatric drugs are (see article: “People with severe mental illness die younger ...”). During this crisis, while he was incapacitated, the staff and other patients stole his belongings. I call this the 'scavenger’s takeover': first, the staff (the lions) take the food and money, followed by the patients (the vultures) who take the clothes and toiletries. They acted this way because they assumed he was dead, or so close to death that he would never return to the ward.
In my opinion, the problem with this patient is not a mental illness, but rather a lack of intellectual capacity — a state shared by many who end up in this hospital, sometimes as a direct result of the drugs they have been forced to take. If one visits the remains of the museum at Mount Carmel Hospital, there is an inscription from over a century ago referring to the facility as an 'Asylum for Imbeciles.' Over time, being ‘intellectually disabled’ seems to have been reclassified as a mental illness. This has become an excuse to overdose patients with pills and injections, which is as logical as expecting a lame person to walk properly simply by giving them medication.
They take advantage of the low IQ of these patients, knowing they are in no position to fight for their rights. Often, these individuals are viewed as a burden by their own relatives — voiceless from the start and treated as a nuisance ('xi dwejjaq ghandi bik'). Trapped in the hospital with nothing to do, they often become heavy smokers, constantly begging for money. This lack of agency allows psychiatrists to conduct blatant experiments on them with total liberty.
The cycle does not stop there. Once a patient is overdosed with a specific injection, psychiatrists experiment further, using additional drugs to 'cure' the horrific side effects of the initial medication. Unscrupulous psychiatrists do not eliminate the source of the problem — their own 'fake' medication — but instead see each side effect as an opportunity for further experimentation.

Consider a typical example: a man loses his job, and as his finances dwindle, he begins to despair. He seeks help from a psychiatrist who, instead of providing relief, adds fuel to the fire by prescribing pills. These drugs carry debilitating side effects (THE DIRECT EFFECTS) such as rapid hair loss — damaging his self-image — and impotence, which creates friction with his partner and destroys his self-esteem.
This gives him even more reason to feel worthless (THE INDIRECT EFFECTS) and sink deeper into despair—especially since depression itself is often a side effect of the medication. This cycle creates a forced dependency on the psychiatrist (THE MONEY-DOWN-THE-DRAIN EFFECT), leading to a constant need for consultations (THE MONTHLY-SERMON BRAINWASHING EFFECT).
Unknowingly, the victim loses control of his mind and becomes a sedated shadow of himself due to the medication, failing to realize he is being blatantly derided, defrauded, and robbed. Once his money is gone and he is reduced to a disabled state — unable to fend for himself and viewed as a 'burden' — they lock him in a hospital. Behind closed doors, they experiment more freely with higher dosages to refine their methods for future victims, likely maintaining close ties with the pharmaceutical industry to further line their pockets. Psychiatry is a fraudulent branch of medicine — a predatory business that exploits the vulnerable. Victims seek help, only to find themselves preyed upon by wolves in sheep's clothing.

When I mentioned that some are reduced to 'imbeciles' as a result of being drugged, I was speaking from my own experience with the INVASIVE TREATMENTS of Fluanxol and Risperdal injections. Before my 2014 arrest, I worked for years as an engineer in a position of significant responsibility without the need for treatment or sick leave. Yet, under the influence of these injections, my mind was rendered practically incapacitated. I experienced a form of induced aphasia (that terrifying disconnect between having a thought and being unable to manifest it) — a total breakdown in the brain's ability to process and communicate language.
To put it plainly: I would have an idea of how to hold my 'consultant psychiatrist' accountable, but the thought would be so short-lived that by the time I picked up a pen, I had no clue what it was. I would sit there, staring at the paper like an illiterate cretin; the simple act of reaching for the pen was enough of a distraction to make my mind forget its purpose. It felt as though my mind was trying to fight back, but the diabolic sedation acted like a FENCE AROUND IT — much like the one installed on the Mosta Bridge — ready to instantly block any progress.
To cope, I would lie in bed with a shirt over my eyes to block out distractions, keeping a pen and paper within reach to jot down key points the moment an idea surfaced. Communication became a humiliation. I would be mid-sentence and completely lose my train of thought, forced to ask, “fuqhiex kont qed inkellmek ghax insejt” (what was I talking about? I forgot). It was embarrassing to feel the person across from me thinking, “kif inhu mohhu spiccut” (his mind is gone).
Imagine trying to fight for your rights in this state. Instead of making your point, you appear incompetent. Rather than exposing the damage the drugs have done, you inadvertently justify their further use. I looked through the leaflets for Fluanxol and Risperdal, but I couldn't find a term that fits this 'induced imbecility' (could it be aphasia, as seen with the poison Olanzapine?). I am convinced it isn't listed because, in psychiatry, reducing a patient to this state isn't seen as a side effect — it is considered a 'healing effect.' It is a sign that the patient is 'responding well' to their malicious aims.
As I said before, entering psychiatry is like getting caught in a cobweb. If someone claims they are doing well on these drugs, it is either their own immune system fighting back or they have been rendered too incapacitated to realize they are being made a fool of. In Malta, we say Iz-zmien itina parir” (Time will give us advice). The only difference is that, given enough time, the psychiatrist buys another villa while the patient has invested only in a coffin and a tomb.

To mention another incident among many at Mount Carmel Hospital, there was a patient, JS, in his 70s nicknamed 'Is-Susu.' If I understood him correctly, he had contracted an illness around the age of 16 that left him with a hunchback, unable to walk upright. He died on October 28, 2016, in Ward MW3A from a heart attack — likely a side effect of those evening pills he had just taken on an empty stomach (just as it had happened to DZ il-Bugan in the same ward two years earlier, on October 4, 2014) or those 100mg Modecate injections he had been subjected to for years, even well beyond the age of 65.
Records show he was also administered 10mg of Kemadrin every fortnight, presumably to combat the severe Parkinsonism induced by his treatment. His tremors were so violent that he could not drink by himself; he would spill almost the entire contents of a cup onto his clothes. I often felt such pity for him that I stepped in to help. Eventually, I cursed the situation as his health deteriorated further; he began asking me to assist him in the toilet — helping him with his trousers and handling the toilet paper — tasks the staff should have performed. At the time, there were few foreign workers, and the Maltese staff seemed to shun the basic care duties they were responsible for.
When he died in 2016, they likely lacked the decency to perform a legally required autopsy to determine the cause of his "inexplicable" death. Psychiatrists can usually play it safe, knowing it is difficult to legally link a death to psychiatric side effects when a patient’s health has been declining for years.
I am convinced his death was yet another case of “Oqtol u idfen” (Kill and bury) at the hands of psychiatrists, with the silent complicity of the hospital staff and authorities. A year or so before he died, he had already been on the verge of death. The nurses had called the hospital doctor, but the doctor refused to transfer him to Mater Dei Hospital. Apparently, staff at Mater Dei had previously accused Mount Carmel doctors of incompetence for "burdening" them with every minor mishap. To avoid appearing like an idiot for the umpteenth time, the doctor left the patient slumped on a sofa in his room — unconscious and dying — for nearly two days. It was only after a nurse finally protested that he was transferred.
My impression is that many doctors at Mount Carmel are so incompetent they wait for nurses to tell them what to do. One patient told me how he complained of chest pains to a newly graduated psychiatrist, who immediately tried to change the subject to "psychiatric trivialities," like whether the patient had slept well. That is the extent of their "expertise." If a patient sleeps well, they do nothing; if he doesn't, they use it as an excuse to drug him further to help him "cope" with pains that were likely caused by the psychiatric medication in the first place.
“Is-Susu” eventually recovered and was sent back to Ward MW3A. I remember him from 2005/2006, when he could still walk — albeit bent sideways. By 2014, he was wheelchair-bound, waiting for his demise. When he had been on the verge of death previously, the staff had already given his room away, assuming he would never return. His substantial collection of village feast magazines, which he had carefully kept in his locker, was dumped into the rubbish. This act proved the staff’s total lack of culture and vision; those archives could have formed a small library within that “Asylum for Imbeciles.”
The most telling part of this story is the contrast between the specialists at Mater Dei — who base their work on scientific tests like X-rays and blood samples — and the psychiatrists at Mount Carmel, who base everything on presumptions. The Mater Dei doctors clearly view the MCH staff as incompetents and “tobba tal-isem” / doctors in name only, who simply offload their problems. In the end, it is always the patient who suffers for their incompetence.

Apart from 'Is-Susu,' there was another patient in MW3A named AC. He was a sort of hunchback, though not in the typical sense; rather than a curved spine, his neck was permanently twisted and bent forward. This was not a natural ailment, but a clear case of Tardive Dyskinesia (often irreversible neurological movement disorder caused by the long-term use of dopamine-antagonist medications, most notably antipsychotics [neuroleptics] like — Fluanxol, Risperdal, and Olanzapine) or Tardive Dystonia (permanent muscle contractions/twisting) — a severe, often irreversible movement disorder caused by the long-term use of the very neuroleptics they force upon us. He was nicknamed “il-Lokus” or “Gamgam.” Being locked in this hospital means more than just risking a premature death from being drugged; seeing the frightening way some patients end up disabled or "reduced" makes it feel like living in an afterlife — a cemetery surrounded by resuscitated zombies.

The patient GM I mentioned previously, who had to use a lawyer to get his dosage reduced, remembered “il-Lokus” from many years ago in a different ward. He insists that, back then, the man's physical condition was nowhere near as severe.
 Some psychiatric “success stories” (sarcasm intended) — the debilitating effects of Tardive Dyskinesia and Dystonia. Patients RB and GM illustrate the severe, long-term harm of psychiatric drug interventions. RB routinely turned to psychiatrist Joe Vella Baldacchino to beg for more medication, a request with which the latter wholeheartedly complied.
Some psychiatric “success stories” (sarcasm intended) — the debilitating effects of Tardive Dyskinesia and Dystonia. Patients RB and GM illustrate the severe, long-term harm of psychiatric drug interventions. RB routinely turned to psychiatrist Joe Vella Baldacchino to beg for more medication, a request with which the latter wholeheartedly complied.
This “Lokus,” seen here in some detail, used to claim he was once a police officer and an amateur boxer. One day, while in church, he allegedly exposed himself. It seems the priest set aside the teachings of Christ to seek total revenge. Without a shred of conscience, the priest wrote to the authorities to have him committed to a mental institution.
Notice the similarity to what I mentioned before: how easy it is to label someone “mental” and then leave “the Psychiatrist to do the rest.” This happened just six days after his 29th birthday. He turned 29 on December 9, 1971, and his "Date of Admission" is listed as December 15, 1971. This is the beauty of delving into history; it gives meaning to what otherwise seem like meaningless dates.
One could guess the obvious: that this act was merely a stunt or a dare — a joke among friends, perhaps for a can of beer and a half-dozen pastizzi. I cannot say for sure what the true reason was, but he certainly paid a high price for it. He has been locked in this hospital ever since — a life sentence handed down by a vile priest who likely exaggerated the facts for the satisfaction of seeing him locked away (biex għaddiet tiegħu). It gave the psychiatrists a perfect opportunity to experiment on yet another victim with drugs and "treatments."
Rest assured, Christ Himself would not have condemned him. However, His inaction in the face of such injustice makes one wonder what kind of God He is, or if He ever existed at all. I will one day recount my own experience: at the height of the abuses in my first court case, I instinctively turned to God for help. When that help never came, I reacted toward the Eucharist in a way that was "a bit much." Later that day, I paid the price: “Is-seqer jiena u nitimgħu wara nofsinhar, nisimgħu għall-ewwel darba jwerżaq għal diversi drabi” (As I was feeding the hawk in the afternoon, I heard it screaming for the first time, over and over again). In the end, it was the psychiatrists and the priest who condemned him — the "whitewashed tombs" that they are.
 The above is an extract from Malta’s Mental Health Act (Part III, Clause 6.1.f), which states that the Commissioner [for Mental Health] can “authorise... scientific research on persons [patients].” This effectively means that many patients in Maltese mental institutions are treated as guinea pigs — in particular those held under a court order, who are stripped of their right to refuse and forced to endure these chemical experiments. They are subjects for drug experimentation, left to the mercy of psychiatrists and the potentially lethal side effects of psychiatric medication.
The above is an extract from Malta’s Mental Health Act (Part III, Clause 6.1.f), which states that the Commissioner [for Mental Health] can “authorise... scientific research on persons [patients].” This effectively means that many patients in Maltese mental institutions are treated as guinea pigs — in particular those held under a court order, who are stripped of their right to refuse and forced to endure these chemical experiments. They are subjects for drug experimentation, left to the mercy of psychiatrists and the potentially lethal side effects of psychiatric medication.

After this extensive account and the listing of so many abuses, I hope that by now one has a clear idea of what psychiatry and its "experimentation" truly involve. As usual, they administer some form of diabolic "pill," drugging and sedating you to strip away the physical and mental ability to ever repeat a perceived wrongdoing. If you dare to persist, they simply continue to increase the dosage or experiment with something new and even more malevolent. It is that simple — an endless repetition of the same story. If they act this vilely today, one can only imagine how much worse it was more than half a century ago.

 Psychiatrist Abraham Galea. In his Valletta office, his desk drawer was reportedly “crammed full with Black & White Whisky, tal-kelb (of the dog).”
Psychiatrist Abraham Galea. In his Valletta office, his desk drawer was reportedly “crammed full with Black & White Whisky, tal-kelb (of the dog).”
In those days, "il-Lokus" was likely a victim of Psychiatrist Abraham Galea — my former neighbor in Mosta and the father of Psychiatrist Ethel Felice. It was Felice, along with David Cassar and Peter Muscat, who fell for my bait by reaching a false conclusion in their report during my 2014 court case.
While I had no direct experience with Abraham Galea, the stories surrounding him are telling. My mother recalls that my aunt, a cleaner at St. Luke’s Hospital, once sought a fraudulent certificate from him stating she was unfit for work. He reportedly complied; she was boarded out and enjoyed taxpayer-funded benefits without ever being prescribed medication for the "illness" he had diagnosed — a testament to how fake the process was. Other former patients recounted visiting his Valletta office to offer "Black & White Whisky" in exchange for favors.
Logic and common sense suggest that being qualified in a field as fraudulent as psychiatry, Galea himself must have been a fraud. As the ancient Romans said: "Falsus in uno, falsus in omnibus" (False in one thing, false in everything). This was even truer in an era when technology was more primitive than it is today. Back then, they experimented in vain to understand the brain; today, they are still experimenting because they still understand almost nothing of this astonishingly complex organ. It is as if the Divine shared many secrets but kept the one that controls everything — the mind — for Himself. Man may egoistically pretend to surpass all, but he eventually realizes there is a power far greater than him. I am convinced that psychiatrists can experiment relentlessly, but they will always remain blatant liars, basing their practice on mere presumptions rather than facts. Even a 2018 article from Psychology Today admits as much with its title: "We Scientists Know So Little About Mental Illness." They know almost nothing, yet pretend to know everything. One only has to look behind the mask.
Psychiatrist David Cassar, listed as "il-Lokus’s" consultant, was likely a new graduate in the mid-80s (having been born in 1961). He would have been learning through direct, "hands-on" experimentation — drugging patients at leisure to discover what "psychiatry" truly means. A man like Cassar would not miss such an opportunity to take things a step further. Having a tyrant trained in this diabolic field provides the perfect ingredients to create the monster he has become.

Don’t ask me why "Is-Susu" and "il-Lokus" managed to live beyond seventy, unlike Mangion and Harrington. I have tried to answer this question before. It could be because the latter two, having come from more violent backgrounds, ended up in conflict with the staff or other inmates; they were more deeply hated. Or perhaps it was the fact that they were locked away for life, forgotten and abandoned by almost all their relatives — voiceless and out of sight. In both cases, it provided an opportunity for them to be drugged at leisure.
But I can give you a hint based on my own experience. While held in Forensic before my sentencing, I was called periodically to appear before the psychiatrist — usually Maria Axiak. In their sadistic pastime of experimenting with drugs, they bombard you with questions in an attempt to make you feel guilty or ashamed. God forbid I should tell them I had nothing to be ashamed of. I had killed no animals — unlike the hunters and trappers in their "traditional pastime" — I merely utilized those already found dead. It is those who actually killed them and kept driving, and the Police who maliciously framed and character-assassinated me to save face, who ought to be ashamed. But saying that would surely be labeled as "poor insight" — a perfect excuse to drug me further.
In other words, you cannot tell them what you actually feel; you must tell them what they want to hear. You have to admit to a "guilt" even if you are guilty of nothing, inventing excuses to lessen your responsibility — claiming you were passing through a difficult time and turned to "unusualities" to boost your morale. I could never tell them that, thanks to those "unusualities," I managed to subject the entire Police force to the most humiliating case in their history without harming a soul.
While their names will die with them, mine will likely survive my death. This was an encouragement given to me by a fellow inmate in Forensic, not a psychiatrist. He told me: “Jien ismi jmut miegħi, int jgħaddu mitt sena u tibqa’ tissemma” (My name will die with me; in your case, a hundred years will pass and you will still be spoken of). Those words meant everything to me during those times when the local media was busy inventing blatant lies. As M.C. Escher said: “Only those who attempt the absurd will achieve the impossible.”
To return to the point: under the guise of “helping you live with remorse,” they diagnose you with depression to justify drugging and experimenting on you. Psychiatrists mask their malice by pretending they want you well, yet "illnesses" like depression are often merely side effects of the pills they prescribe. They intentionally make you mentally ill to create further excuses to drug you.
NOT TO BE HANDLED BY THE PATIENT ...

In a country as historically corrupt as Malta, one should expect laws to be drafted for the benefit of the privileged and the high-ranking, while remaining discriminatory against us "mere mortals."
For example, when Value Added Tax (VAT) was introduced years ago, a small-town ironmonger selling a €1 can of paint for a meager 5-cent profit was put through a nightmare if he dared fail to issue a receipt. This was not the case for doctors and lawyers — the professions of most politicians — who were either exempt or simply did not have the tax enforced on their far more profitable services.
Similarly, successive corrupt governments have allowed doctors in the public sector the privilege of writing whatever they wish behind your back in your hospital file. If they happen to misdiagnose you, they have the support of a corrupt state and authorities who are always ready to provide cover for their malpractice and experimentation.
This is a corrupt practice rooted in the past, when science and medicine were still in their infancy. If a doctor had no clue why a patient — perhaps your grandfather — was complaining of back pain, rather than appearing incompetent, he would invent a diagnosis. He would pretend to understand the ailment just to pocket the fee, prescribing medicine that often did far more harm than good — treating a simple muscle strain as though it were severe arthritis.
I am referring to the image above showing the cover of my Mount Carmel Hospital file, marked with those vile words in block letters: "NOT TO BE HANDLED BY THE PATIENT." In their twisted mentality, breaching this rule must be the one unforgivable sin that even Christ Himself could not absolve. After all, why should a "guinea pig" of a patient interfere with what an "intellectual" fake doctor has decided to drug him with?
Your hospital file is at the full disposal of the staff to feast upon, yet you, the "miserable patient," are denied access to what has been written about you or the labels they have pinned on you. It is "Data Protection" in reverse: outsiders have full access to your personal history, while you, the victim, have no protection and no access to your own most intimate information.
While a defender of the system might claim this is to prevent a patient from becoming "depressed" by reading the file, the true diabolic intent is far more calculated. It protects the "privileged" liar while leaving the patient disadvantaged from the start. If you dare ask to consult your file to hold a doctor accountable, the authorities will not only tip him off but grant him the time to destroy evidence — tearing out pages or making the entire file vanish, as happened in my case — only to replace them with forgeries. He may even take it a step further, accusing you of defamation while you are left empty-handed and destined to lose in court.
The file is kept hidden not for the patient's health, but to ensure the doctors remain covered by a corrupt state. What other purpose is there for hiding a diagnosis if not to cover up incorrect conclusions and blatant lies? That phrase — "NOT TO BE HANDLED BY THE PATIENT" — is black-on-white proof of something intentionally malicious. It is kept hidden as if it were occult (from the Latin occultus, meaning to hide or keep secret).
This confirms a terrifying reality: the State is fully aware of the corrupt practices and drug experimentation carried out by psychiatrists. By granting them this privilege of secrecy, the State ensures their impunity. This is the face of institutionalised corruption in Malta. It is like telling a thief to rob a bank’s customers while intentionally switching off the CCTV. By denying the patient access to their own file, the State effectively "switches off the cameras," making it almost impossible to incriminate the psychiatrist. This privilege has been exploited for decades, allowing these "doctors" to focus on their sadistic pastime of experimentation — likely fueled by "extra salaries" from the pharmaceutical lobby at the expense of the patients' lives.
It is another example of exactly what was pointed out in the opening paragraph of this webpage: “Psychiatry involves an unequal power relationship between doctor and patient.” This imbalance of power allows even the most blatant lies invented by psychiatrists to be treated as sacred truth. In contrast, any evidence, factual data, or witness testimony a patient provides is dismissed as doubtful or a waste of time.
To make matters worse, as noted in this link regarding corruption in Malta, hospital policy dictates that medical records are destroyed ten years after a person's death. This ensures that they not only make it difficult to obtain evidence against them during your lifetime but effectively eliminate that possibility entirely at the first opportunity.

Psychiatry, much like fortune-telling, is a massive, fraudulent enterprise on an even larger scale. As the saying goes, "wherever there is a vast amount of money, someone, somewhere will be up to no good." The "NOT TO BE HANDLED BY THE PATIENT" label highlights a systemic fraud. It is as if one football team (the psychiatric profession) bribes the opposing players (politicians) and the Football Association (authorities) to secure a trophy — pocketing money through a fake profession and unscientific diagnoses — even though they do not deserve it. Instead, they ruin the lives and health of their patients while regulatory boards, such as the Medicines Authority, manipulate standards to allow such deplorable acts, approving diabolical drugs and injections with frightening side effects like Parkinsonism.
As the ancient Romans said, “Radix omnium malorum est cupiditas” (Greed is the root of all evil). Given the insatiable greed of psychiatrists — many of whom juggle multiple roles to pocket several salaries — I am convinced that the profession represents a unique level of harm. They create victims who are silenced, discredited, and disabled. In such a state, it feels as though only divine intervention could restore a person, as the world remains blinded to these abuses, leaving the victim to suffer in silence, abandoned to their fate. I may be a staunch atheist, but I hold this conviction with total certainty. Psychiatry, much like other powerful institutions, remains shielded from criticism because it is backed by the immense wealth of the pharmaceutical industry.

As another example of the sadism inherent in psychiatry, imagine the world’s brightest scientists and engineers tasked with investigating an airplane crash, despite communication with the aircraft having been lost long ago and the black box never being found. Without instruments or data, they are no better informed than a person on the street. If it happened to be raining that day, they might allude to bad weather as the cause, even if the crash was actually the result of sabotage.
Psychiatry operates in much the same way. Despite the era we live in, the field remains in its infancy — and I am convinced it will always stay there. With practically no instruments or objective science to determine with certainty that someone is suffering from a specific mental illness, they must base everything on mere presumptions — and often blatant lies. This is never a problem for them, however, as long as it continues to fatten the pockets of those in this fraudulent profession.
The warning "NOT TO BE HANDLED BY THE PATIENT" is telling. If they consider it a "sin" for the file to be handled by the patient — whom they have already disadvantaged by discrediting them as "mentally ill" — imagine how much more they fear that file being handled by someone wise enough to incriminate them and expose their fraud. To take it a step further, having experienced abuses from both psychiatrists and the police, I see "NOT TO BE HANDLED BY THE PATIENT" as the psychiatric version of a police frame-up. They attribute "wrongdoings" (illnesses) to you that they know for certain you did not commit (diagnoses you do not have), creating a truly impressive and disturbing similarity between the two.

Consider my own case as an example. If I dared to request access to my files from the authorities, they would immediately notify the very person I am seeking to incriminate: Psychiatrist David Cassar. As explained previously, such an effort would be in vain. He would have the time and power to destroy or manipulate evidence — or simply make it vanish, as happened with my second court case and my hospital file. Those documents incredibly disappeared despite being under the court's jurisdiction and guarded by CCTVs, metal detectors, and officers.
Furthermore, being the tyrant he is, he would manipulate my suspicion of his wrongdoing — a natural reaction to his malpractice — and frame it as a symptom of “delusions of persecution.” Because psychiatry is a profession often built on the manipulation of facts, he would use my attempt to find the truth as a desired excuse to sedate me further. Rather than the authorities helping me hold him accountable, the system allows him to destroy me even more.
In the field of psychiatry, a patient who is stigmatized, silenced, and reduced to a "psychopath" is no match for a psychiatrist exalted as an unquestionable expert. To fight for your rights against their many wrongs is invariably labeled as a "total lack of insight" or "inappropriate beliefs." In fact, David Cassar labeled me with these exact terms on several occasions simply because I began reporting him to the Medical Council. They treat the pursuit of justice as a form of severe paranoia, using it as a justification to experiment with increased dosages or other diabolical drugs. You are not even given the chance to speak, let alone present evidence; you are ignored and prejudiced not just from the start, but before you can even begin.
When a victim points a finger at a psychiatrist, they find themselves overwhelmed by "cannons" pointing back at them from every direction. Everyone backs the doctor. They doubt your evidence and facts, yet find nothing suspicious about a profession based on presumptions rather than scientific basis.
This dilemma is even more magnified in a country like Malta, which has long struggled with corruption. In psychiatry, your condition is considered “under control” only once they have silenced you and reduced you to a physically and mentally disabled state. Once that is achieved, they simply turn their attention to their next victim.

Once labeled "mentally ill," you cannot even claim to be sane, for they will instantly reply: “Sometimes our illness prevents us from realizing we are actually ill” (Xi kultant ma nirrealizzawx li aħna fil-fatt morda). They use this “lack of insight” excuse to drug you further, discrediting any evidence you bring by claiming, “Because he is sick, he doesn't know what he is saying; he is imagining things” (Għax dak marid, ma jafx x'inhu jgħid; qed jimmagina l-affarijiet).

Because psychiatry has always been a fraud, you must always look for the opposite meaning in their terms. What they define as a patient’s "lack of insight" is actually their own "abundance of pretension." They pretend to be professors capable of diagnosing mental illness, yet they lack the basic intuition of a child; they cannot even detect when a patient is intentionally misleading them to expose their incompetence.
Imagine visiting a fortune teller who begins asking you questions in an attempt to predict your future — rest assured, he cannot even predict his own. If you were to intentionally feed him lies, he would take the bait and reach false conclusions, proving his own fraudulence. A psychiatrist is no different from a fortune teller. Both exploit their victims to satisfy an insatiable greed for money, and both operate under a disguise: the former pretends to be a medical doctor, while the latter claims to possess supernatural powers.
Both are entirely fake and lack any scientific basis. The psychiatrist cannot rely on even the most sophisticated brain scan, while the fortune teller is reduced to reading the wrinkles on a palm. In both cases, one would have to be either desperate or incredibly naive to waste money and trust their life to such blatant fraudsters. The legal maxim “Falsus in uno, falsus in omnibus” (False in one thing, false in everything) perfectly describes a profession that can be so easily manipulated into reaching the wrong conclusion.

Above from a facebook post.

Above further clarified it myself (eg. Prozac: they said it was safe).

If anyone understands the extent of psychiatric fraud, it is the psychiatrists themselves — much like a liar, a fraudster, or a corrupt politician knows they are deceiving others long before anyone else realizes it. To maintain this deception, they use charming voices or seductive smiles to effectively hypnotize their victims, much like the leader of a dangerous cult. Their goal is to coerce the victim into believing they are mentally ill and in need of fraudulent medication. Essentially, they attempt to transform their own illusions — where they see everyone but themselves as sick — into a perceived reality, turning blatant lies into "facts."
When they encounter someone too obstinate or too wise to fall for their bait, they resort to prescribing injections to force a state of compliance. They justify this by claiming the patient suffers from a "lack of insight" and would stop taking their pills if left unsupervised. By using these diabolical injections and exploiting the "lack of insight" narrative, they prevent you from ever proving two things: first, that you were incorrectly diagnosed, and second, that you were perfectly healthy without their so-called "cure."
While you are on pills, you still have the theoretical power to stop the medication and remain healthy as proof of their error. However, once you are forced onto an injection, they effectively silence you; you can no longer claim your health is due to a lack of medication. It is similar to being locked up: it becomes useless to claim you would behave well on the outside, as they simply argue that your good behavior is only due to being under their constant watch.
This is precisely what happened in my case, except that those injections were administered too late to prevent them from falling into my trap. In their roles as court experts, they reached the wrong conclusions in their reports, attributing my "wrongdoing" to my having stopped the medication — pills which, in reality, I had never taken from the very beginning. This exposed them as complete frauds.
The YouTube video above shows an individual attempting to hypnotize his viewers — setting aside the actual merits of the video, which happens to be an argument against the legalization of divorce in Malta. He uses a "charming," charismatic voice, behaving as if he were some high priest or Messiah. His glasses imply he is well-read and, by extension, suggest a higher intelligence; meanwhile, his white beard seems calculated to make him appear as an old man full of life experience — perhaps even a modern-day Socrates or an ancient Greek philosopher.
This man is none other than psychiatrist David Cassar. If you happen to hold a different opinion on divorce than this "unquestionable expert" (who clearly thinks he knows better than everyone else), he would likely conclude you are suffering from a "lack of insight." To him, you surely need a fortnightly prescription of that diabolic injection, Risperdal Consta, to regulate the dopamine supposedly missing from your "sick and psychopathic" mind.
The video above, a screen capture of my laptop, shows the Facebook page of a certain Anton Grech, nicknamed "Malta's Lino Banfi". He employs a different method of hypnosis: his seductive smile (or as we say in Maltese, "jikxef sninu" — revealing his teeth). He frequently appears on television, indoctrinating his "flock of sheep" with absurdities and presumptions. While he once claimed that photography is his hobby, that was clearly just for the airwaves; his true pastime appears to be being photographed.
He seems to have a "slave" or lackey at his disposal 24/7, tasked with taking photos for his Facebook albums. While a few photos of him smiling might be acceptable, the sheer multitude of them reveals his true personality: a self-glorifying ego reminiscent of Stalin’s cult of personality in the USSR. As a psychiatrist by profession, I suppose Anton Grech finds much to laugh about — especially at the expense of the lackey following him around.

Once you are labeled 'mentally ill,' you become entangled in a web that you can never dream of escaping. You are forced to let them drug you and experiment on you under the pretext that only their 'diabolic' drugs can keep your condition under control.
Because psychiatry is so flawed, you can’t expect a psychiatrist to ever actually cure you. It’s not like recovering from a fever that lasts a week. Instead, almost every diagnosis they give is labeled 'chronic.' For example, if you find a job, they claim you'll remain depressed because you are bullied for your label, or because you can’t cope due to the way they have sedated you.
Once labeled, you stay that way forever — a voiceless slave and a guinea pig without rights, always at their disposal. Thanks to psychiatry, we are reliving the dark days of the Middle Ages: a time when the masters gave the orders and the sheep had to follow; when you owned nothing, not even your own life, and everything was dictated for you by a privileged class.

While the patient in psychiatry ends up a victim — a guinea pig experimented on with "diabolic" drugs at the leisure of the system — for the true criminals, it is big business. This includes many psychiatrists themselves (ask Mangion and Harrington, if only they could speak from the grave). For the privileged class, psychiatry is a blessing, used as a tool for "crime-laundering" to cover up corrupt practices.
A prime example is Magistrate Carol Peralta. Through the blatant lies of psychiatrist David Cassar, who labeled me "mentally ill," Peralta managed to transform his courtroom threats — of "smashing me against the wall" — into my own "delusions of persecution." This allowed him to escape accountability and retire from the judiciary with honors, despite some criticism for his eccentricities. Do not expect much from our legal system; even the Commission for the Administration of Justice, the supposed watchdog, covered up Peralta’s blatant abuses. In a country that has always been corrupt, the law exists only for us mere mortals, while the privileged and the "friends of friends" are always excused.
Take another example: the sons of former Deputy Police Commissioner Raymond Zammit. Like father like son, they proved themselves incompetent and unworthy of the uniform. After falling under inquiry for irregularities — including the Gaffarena-Zammit scandal — they were "boarded out" under the excuse of psychiatric illness. This further confirms that psychiatry is a total fake. Suspiciously, this happened just before inquiry conclusions were released, allowing them to qualify for a life pension they would have lost if they were expelled. (Much like how Magistrate Peralta "retired" in 2015 to save the Commission the embarrassment of dismissing him).
Of course, these people never spent a single day locked in Mount Carmel Hospital for their "illnesses." In fact, just four days after one was boarded out as unfit for work, he was given a €60,000 job at Enemalta under Fredrick Azzopardi — a salary equal to three or four common workers. The appointment was only cancelled after the case went public.
This is just the tip of the iceberg. As the Latin proverb says: “Falsus in uno, falsus in omnibus” — false in one thing, false in everything. If you wish to ruin your life at the hands of psychiatrists and psychologists — who hide behind bombastic titles like "Practitioner," "Counselor," or "Consultant" — remember that behind the mask, they are nothing more than fortune tellers. They have no scientific basis to prove you are "sick."
Psychiatry is not a science; it is based on presumptions. Rather than admit the truth and risk their jobs, they fatten their pockets by exploiting the vulnerable. They make you dependent ("see me in a fortnight"), keep you trapped forever ("it’s a chronic illness; pills for life"), and experiment on you ("let's try this pill"). When you experience side effects, they simply drug you further say with Artaine or Kemadrine. Never expect a cure from a profession that has been a fraud from the start ("Sometimes, we don’t even realize we are unwell" / "Over time, it is better to increase the dosage as the body builds up a tolerance.")

For further evidence of how fraudulent psychiatry was, is, and will surely always remain, look at this article from The Washington Post: 'This secret experiment (namely, the Rosenhan Experiment) tricked psychiatrists into diagnosing sane people as having schizophrenia.' The article tries to sugarcoat the reality by claiming, 'this is far from how mental-health care is practiced these days.' I strongly disagree. Even if there have been some positive developments in the USA, psychiatry in Malta remains as oppressive as it has ever been.
As a reminder, consult Schedule 14, Part 2 regarding the 'Application for Invasive or Irreversible Treatment.' In Malta, it is dangerously easy for psychiatrists to proceed once they have an Order Number in hand (such as a CDO – Continuing Detention Order, or an EIATO – Extension of Involuntary Admission for Treatment Order). As for the claim that 'consent is in writing and signed by the person,' I will explain further below — based on my own harrowing experience — what that actually means in practice.
I compare psychiatry to circumcision — an irreversible procedure performed on minors who cannot decide for themselves. Much like the vulnerable patients falsely discredited as 'mentally ill,' these children are subjected to a practice falsely promoted as beneficial to health. The World Health Organization even claims there is 'compelling evidence' that male circumcision reduces the risk of heterosexually acquired HIV by approximately 60%. I suggest that those men foolish enough to believe such nonsense test that theory themselves with HIV-infected partners. When they inevitably contract the virus, they shouldn't seek answers from the WHO; they should seek a psychiatrist to 'cure' their stupidity and further poison them with psychiatric drugs. They would certainly deserve it.
As for mental institutions, I compare them to an orphanage where the custodians are predators who find satisfaction in abusing the children. In this metaphor, the 'children' are vulnerable patients, and the 'abuse' is the drugging and experimentation that leaves them traumatized and destroyed. To the outside world, these custodians appear caring and devoted; yet within the walls, the reality is a different story. Patients are punished — drugged further — for the slightest mishap, such as daring to report staff abuse. If they speak out, they are immediately dismissed as having a 'lack of insight.'
Just as there is a stigma toward orphans for their background, psychiatric patients are stereotyped and labeled for life as 'insane' or 'voiceless.' Their words are always taken with a grain of salt. However, the power of a psychiatrist — no matter how much of a liar he may be — far exceeds that of an orphanage custodian. Once labeled 'mentally ill,' you become more voiceless than a five-year-old. The world will listen to the allegations of a child, but they will ignore the evidence and facts provided by a university-educated professional, simply because they have been branded with a psychiatric label.
In fact, it seems we have a court system and a police force with upside-down priorities. We saw one sent to prison for over a year based on the false testimony of his daughter; meanwhile, I have built a website filled with 'black and white' evidence, yet the police refuse to intervene. I have suffered immensely because Malta has such a void in investigative journalism, allowing those in high positions to persevere in their abuses with total impunity.
There is a stark contrast in what the authorities find concerning. They would rightfully act if a custodian placed a hand on a child, yet they show no concern when a patient is locked away and abused for years by a psychiatrist. These patients are destroyed by the side effects of psychiatric medication — suffering from depression, parkinsonism, sterility, and sedation — reduced to a state where they have no control over their own minds or selves. The 'big business' behind psychiatry mutes everyone.
I remember a remark a nursing aide once made to another: 'L-ewwel it-tobba lill-pazjenti jaraw kif joqtluhom, u mbaghad irridu nza*bu bihom ahna' — 'First, the doctors find a way to kill the patients, and then we have to deal with the mess.'
Once you are labeled 'mentally ill,' you become meaningless and stripped of your rights. Your cries do not even reach the volume of a whimpering puppy. A patient in a mental institution is treated worse than an animal — like an ant facing ferocious lions. Those behind psychiatry are often psychopaths themselves, without scruples or conscience, fattening their bottomless pockets on presumptions and blatant lies. They are always on the lookout for their next victim to label and exploit.
Hence the Latin saying, 'Lucrum sine damno alterius fieri non potest' — 'Profit cannot be made without another’s loss.' In psychiatry, the patient's loss of health has always been the psychiatrist’s financial gain. It makes one wonder exactly why Psychiatrist Anton Grech has so much to laugh about in the video above.

But didn’t I mention in the previous paragraph that the massive business interests behind psychiatry tend to silence everyone? At one point, I was in contact with Sandra Gauci, who frequently uploads videos discussing trending topics. Around July 2021, I wrote to her regarding the victims of psychiatry. As shown in this email thread, she replied on August 12, 2021, at 3:14 PM with the following (translated into English):
“I found someone else who was also a victim of your doctor (Psychiatrist David Cassar). I am trying to convince him to testify. His brother died from the medication he was prescribed. I will keep you updated, as the person involved wants justice, which will work in your favor. For now, I am not disclosing anything further, but you are not the only victim. At least you are still alive.”
However, this glimmer of hope was short-lived; I never heard from her again. As the Latin proverb says: Curae leves loquuntur, ingentes stupent — “Light griefs speak, but deeper sorrows are silent.” It is a tragic reality for the many victims of psychiatry who are left abandoned to their fate. To the system, another death is of little consequence; what truly matters to them is suppressing anyone who dares to speak out.

In the images above, I am standing in what used to be the clinic of Male Ward 3A, a few weeks or perhaps months after it was closed in late October 2019. In the first photo on the left, one can see the board that used to list the patients' names. The photo on the right shows this same board with the names of the last four remaining patients; one of those is mine, which I have indicated with an arrow. You can see from the window behind me that it was likely quite dark outside, but at least I was there in time — just days before they cut the electricity to the entire block around January 9, 2020.
It is possible that the staff of my new ward, where I was eventually transferred, were being paid to nap from 10:00 p.m. until 5:00 a.m. the following morning, or perhaps they had simply closed the ward early to sleep while they were supposed to be on duty. The Maltese public criticizes people like Theuma for receiving a three-month salary without reporting to work, yet they applaud these staff members as "national heroes" — despite them being paid to sleep since time immemorial. (I will exclude the nurses at Mater Dei, who perhaps do not stoop to such levels and only spend "a few hours" sleeping or chatting behind the desk). Of course, they cannot dismiss the staff of this ward, because they would then have to dismiss the entire hospital staff for doing the same or worse.
In fact, it is customary in most wards of this "fake" hospital to lock the dormitories and prevent patients from going to bed during the day (except for two hours after lunch). This ensures patients are tired enough to sleep through the night so as not to bother the night shift, even though most patients are already sedated enough to be incapable of doing otherwise. Consequently, you will often see patients sleeping on sofas or even on the floor during the day. This is never a problem for the staff; it is only a problem for the patients. The staff constantly try their utmost to make the patients' lives even more miserable and boring, all so they can enjoy a deep sleep and wake up refreshed enough to handle their private jobs and daily errands.
As always, the patient — the underprivileged class — is blamed, while the staff — the privileged class — are excused in a country as historically corrupt as Malta (see below for the revenge they took on me for reporting staff sleeping through the night). In these photos, I am taking a form of revenge by standing behind the desk of the MW3A clinic. This is the same desk where they recorded the administration of my 65th consecutive injection (out of 67 total; the first two were administered in the Mixed Admission Ward). That diabolical, invasive treatment made my life a living hell.
Given the state of this corrupt country, the hospital staff surely deserve the "Ġieħ ir-Repubblika" award for their "commendable" work: remaining silent in the face of abuse, ruining patients' health with psychiatric medication during the day, and ensuring patients are sedated enough at night to never interrupt their sleep. And if a patient isn't sedated enough, there is always an "emergency" injection (Ativan? Valium?) at the staff's disposal — sedating them so heavily that they wake up the next morning soaked in their own urine.
Regarding the absolute mess seen in these photos of the former MW3A clinic, it was certainly not a patient who left it in that state. However, given my history, I expect nothing less than a setup. I was framed for harming and killing animals I had merely found dead on the road; I was accused of violating tombs for simply entering my hometown's church crypt to take photos and measurements; and I was accused of trespassing for entering the cave under the Speranza chapel to take photographs. Therefore, I fully expect the police of such a corrupt country to frame me once again, claiming I am responsible for this wreckage.
The gullible public would surely believe it; once you have been discredited as "mentally ill," any lie they invent about you is easily accepted. But believe it or not, that mess was created by none other than the administration of this "fake" hospital. They sent their "cannibals" to ravage what was once an entire three-story block. This block housed two wards with a total capacity of 80 patients (roughly one-fifth of the hospital’s capacity, who were shifted to private homes — a subtle form of privatization), an archive, stores, and an "Outreach" office. This destruction was based on a completely fraudulent report by an architect who, after a mere visual survey, condemned the entire block for demolition instead of recommending the minor repairs needed for a small section of the roof.
While I mentioned that the police might frame me for the physical mess, the psychiatrists are always a step ahead when it comes to blatant lies. I suspect they will interpret my venture there as evidence of "poor insight" — claiming I failed to realize I shouldn't have "trespassed" to take these photos and videos. In reality, I took them so everyone could see the corrupt practices occurring in this hospital at the taxpayers' expense. The psychiatrists are pushing for a new psychiatric hospital near Mater Dei simply because they want the same status as medical doctors; that alone should give you a clue about the massive fraud behind all of this.
My Experience with Psychiatry: A Tool of Submission to Silence Dissent, Covering Up Crimes Through Forced Medication for Sicknesses Invented with a Stroke of a Pen, and Intimidating the Voiceless with Abusive Detention and the Frightening Side Effects of the Medication Itself.
The accounts above were the experiences of others, for which I literally risked my neck (as they say in Italian, “ho rischiato il culo”) to piece together the stories of a few of the many victims of psychiatry. I did this by photographing relevant documents and, in some cases, taking even greater risks by accessing the original files, complete with fingerprints. God forbid I had been caught red-handed; I would have paid for it dearly with a newly prescribed injection. They would have certainly diagnosed me as suffering from some “extreme form of schizophrenia with a severe obsessive disorder against psychiatry, psychiatrists, and the rest of the scum like psychologists.” This would have triggered immediate and drastic measures using their usual diabolical drugs — specifically, a multitude of not only invasive but also irreversible treatment orders. These are issued by our very own Courts, where injustice and discrimination are often the order of the day for us mere mortals — though certainly not for the privileged class.
What follows is my own personal experience with psychiatry (the full story can be read in much greater detail by clicking the banner at the top). It began with my first court case in 2001, when Psychiatrist David Cassar first tried to sedate me with pills to prevent me from uncovering the abuses I had suffered at the hands of people in high positions:
- Monday, 18-Feb-02: I was prescribed Anafranil (25mg) during my first appointment with Cassar. This was exactly two weeks after that infamous court sitting on Feb 4, 2002, when Magistrate Carol Peralta threatened to smash me against the wall in the courtroom. It had been more than eight months since Cassar was nominated by Peralta himself on June 15, 2001. Initially, these appointments were held on Mondays at Saint Luke’s Hospital
Imagine you are a student who goes to the headmaster (Cassar) to report abuse by a teacher (Peralta). Instead of taking action, the headmaster covers for the teacher and tells you to take pills to sedate you and shut you up. It is like being handed a revolver and told: "Test this on your head; follow my advice, give it a try, and everything will be fine." Would you be foolish enough to follow such malicious advice? Of course not, and neither was I. - Mon 04/03/02: 4x Anafranil (25mg)
- Thu 14/03/02: Pharmacy of Your Choice entitlement approved, fraudulence establishing this as the "Date of first diagnoses" for schizophrenia.
- Mon 25/03/02: 4x Anafranil (25mg), 3x Stelazine (1mg)
- Mon 22/04/02: 2x Anafranil (25mg), 2x Stelazine (1mg)
- Mon 20/05/02: 3x Anafranil (25mg), 3x Stelazine (1mg); however, this time he refused to provide the prescription in writing.
- Mon 10/06/02: I was scheduled for an appointment but did not attend. I had informed David Cassar beforehand that I would skip the session if he did not provide the written prescription from the May 20th visit. He failed to do so. The retaliation was immediate: within two days — and only days after my lawyers had abandoned me — Peralta and Cassar hastily convened a court sitting to abusively lock me up in the hospital.
From June 12, 2002 (the day I was confined to Mount Carmel Hospital, Ward 10) until June 21, 2002 (the day I was seen by three psychiatrists, including Cassar), I was under no medication. Despite this unexpected trauma, I behaved perfectly and showed no symptoms of mental illness. - Sat 22/06/02: 2x Stelazine (2mg) + 2x Artane (0.5mg). This was the day after the evaluation by the three psychiatrists. Note that although I was locked up on the pretext that my “delusions” were increasing, Cassar was actually forced to lower my dosage compared to the May 20th levels because I consistently behaved well. (The dosage was even lower than those of March and April 2002). As for the Artane, it can be ignored; it is only prescribed to combat the side effects of the other drugs, such as restlessness.
- Fri 05/07/02: 1x Risperdal (2mg), increased to 3mg as of July 8th.
- Fri 12/07/02: 1.5x Risperdal (2mg) + 1x Artane.
- Fri 19/07/02: 2x Risperdal (2mg) + 1x Artane (my final day of a 37-day confinement in 2002).
- Fri 16/08/02: 1.5x Risperdal (2mg) + 1x Artane. Once I was released in 2002, appointments were held on Fridays at the Mixed Admission Ward (MAW) at Mount Carmel. This continued until the appeal sentence on Nov 21, 2005, when I was locked up again for exactly two months until Jan 21, 2006.
- Fri 06/09/02: 1.5x Risperdal (2mg).
- Mon 05/05/08 (or shortly before): 1x Risperdal (2mg). After my release on Jan 21, 2006, appointments returned to Mondays at Saint Luke’s Hospital. They later transitioned to Mater Dei Hospital once it opened and Saint Luke’s closed.
- Sat 22/03/14: 1x Risperdal (2mg) + 1x Paroxetine (10mg). This was after I was locked up again, this time in the Forensic Ward at Mount Carmel Hospital following my second arrest on March 19, 2014. The person who began administering these pills was Psychiatrist Maria Axiak. In this photo, she is seen with one side of her head shaved — attempting to cover it by combing hair over from the top. Imagine a man going out with only half a beard shaved; for a doctor to present themselves this way is even worse.
Despite listing herself as a criminologist, she acted with total lack of professional integrity. She began drugging me with psychiatric medication from the very start — long before the court-appointed psychiatrists had even seen me. This was further proof that my case was prejudiced from the beginning; they maliciously intended to label me as "mentally ill" once again. Furthermore, by drugging me, they ensured that when I finally saw the psychiatrists, I would not be in full control of my faculties to explain the intricacies of my first court case. Regarding Paroxetine (also known as Paxetin or Seroxat), it is used to treat depression. Notably, depression is a side effect in more than 1 in 10 cases for that diabolical injection, Risperdal Consta (the depot form of the Risperdal pill). Axiak knew full well she was intentionally inducing depression with the Risperdal, and was essentially experimenting on me with Paroxetine to combat the very side effects she caused. - Thur 17/04/14: 1x Risperdal (2mg) + 1x Paroxetine (10mg) + 1x Tryptizol (20mg). (I cannot recall if the Tryptizol was in addition to the Paroxetine or a replacement). Once again, Maria Axiak, likely alongside Psychiatrist Hector Cutajar, was experimenting on me. Tryptizol is another drug used for depression — a direct consequence of the Risperdal they forced upon me. This is how they "gain experience" in their diabolical profession.
Yet, despite their attempts to drug me from the moment I entered the Forensic Ward and their intentional efforts to make me clinically depressed, I succeeded in outsmarting them. I led no fewer than five "court experts," including David Cassar himself, into a trap. I caused them to reach entirely wrong conclusions in their court reports — final proof of how fraudulent they truly are. If I managed to humiliate these so-called experts while drugged, imagine what I am capable of when I am not. Without harming a soul, I managed to subject the entire Police Force to the most embarrassing and humiliating case in their history — a record that will stand for all time. - Fri 27/06/14: 1x Risperdal (2mg). This was the day after the court sentence was handed down. I was seen by Psychiatrist David Cassar, and if I remember correctly, he kept me only on the Risperdal pill and removed all others. This was merely intended to "sugar the pill," as he already had it in mind to begin drugging me with an injection.
- Fri 08/08/14: Fluanxol (Depixol) Injection/Depot. They began administering this diabolical injection, which carries dreadful side effects (see further below for the record of dosages and dates I was forced to take it).
- Thu 14/08/14: Fluanxol (Depixol) Injection + 2x Artane (2mg). Artaine is used to treat the symptoms of Parkinsonism and restlessness. The Fluanxol made me so severely restless that I was constantly swinging like a pendulum; it was so extreme that Cassar eventually had to reduce the Fluanxol dosage to just 20mg every four weeks. Despite this, I remained almost completely disabled by the constant restlessness.
- Fri 31/10/14: Fluanxol (Depixol) Injection + 1x Paroxetine (10mg) + 2x Lexotan (3mg) + 2x Artane (2mg). Again, both Paroxetine and Lexotan are used to treat depression — another known side effect of that diabolical Fluanxol injection. It is possible the Artane dosage was increased further at this time.
- Sat 29/11/14: Fluanxol (Depixol) Injection + 1x Paroxetine (10mg) + 2x Lexotan (3mg) + 3x Artane (3mg). Note that they did not remove the source of the side effects that were making my life a living hell; they did not stop the Fluanxol. Instead, for their own pleasure — as if they were playing a game — they saw it as an opportunity to continue vilely experimenting on me by prescribing different and additional pills to combat the dreadful side effects.
It is like being repeatedly beaten with a metal rod, only for your attackers to experiment on how to cure the wounds they inflicted. In psychiatry, they first intentionally make you sick, and then they experiment on you, trying in vain to treat the symptoms they caused. They vilely tell you, "Let me give you this pill; maybe it will help you" ("Ħa ntik din il-pirmala, forsi tgħinek").

- 30/04/16: Risperdal Consta Injection/Depot. They began administering this equally diabolical injection, which also carries dreadful side effects (see the record of dosages and dates below).
- 17/12/17: Olanzapine (5mg). Cassar actually intended to put me on the Olanzapine (Zypadhera) injection, but it seems the authorities did not approve his request due to its high cost. Consequently, he began giving me this pill as its equivalent. I would have truly become a guinea pig — forced to endure three different types of injections in just three years.
- 05/04/18: Olanzapine (10mg). He vilely doubled the dosage — a 100% increase — simply because I took photos to uncover staff abuses. (Details of how this happened are provided further below). In this hospital, if you dare to report staff misconduct, you suffer the consequences through your own health; you are drugged, sedated, disabled, and systematically destroyed.
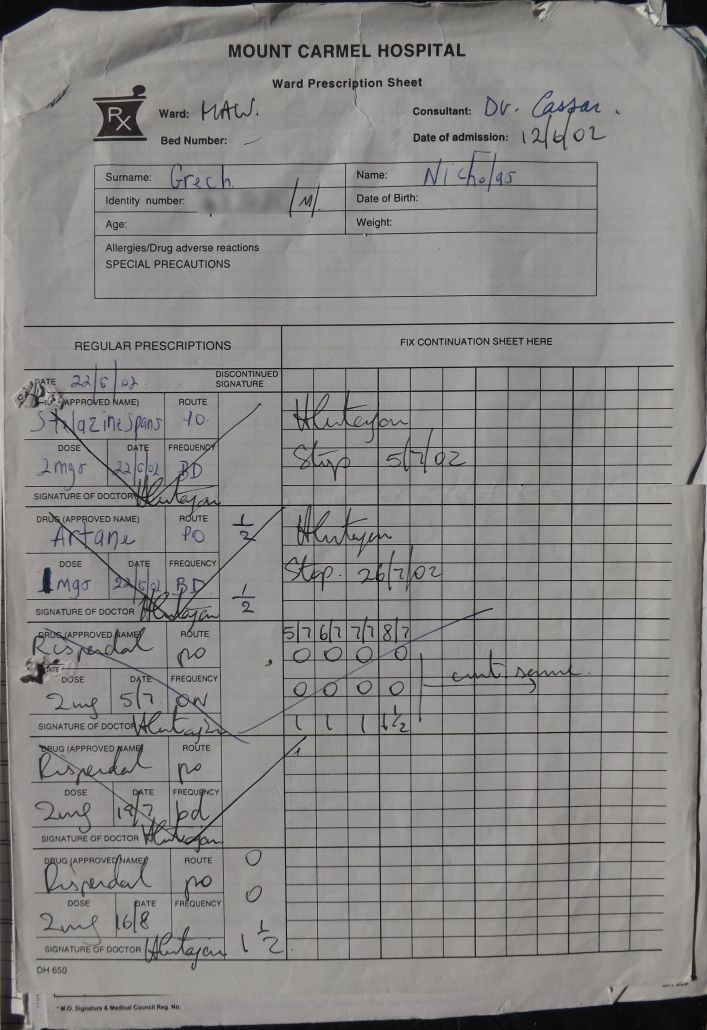{kind=link}
| The following are the dates and links recorded when I was administered that diabolical Fluanxol (Depixol) injection/depot: | ||
| 08-Aug-14 | Fluanxol 10mg | Test Dose |
| 14-Aug-14 | Fluanxol 10mg | Right Arm, 1 week later |
| 28-Aug-14 | Fluanxol 30mg | Left Arm, 2 weeks later |
| 11-Sep-14 | Fluanxol 30mg | Left Arm, 2 week later |
| 02-Oct-14 | Fluanxol 30mg | Left Arm, 3 weeks later |
| 30-Oct-14 | Fluanxol 30mg | Right Arm, 4 weeks later |
| 29-Nov-14 | Fluanxol 20mg | Left Arm, 4 weeks later, etc. |
| 22-Dec-14 | Fluanxol 20mg | Right Arm |
| 24-Jan-15 | Fluanxol 20mg | Left Arm |
| 21-Feb-15 | Fluanxol 20mg | Right Arm |
| 21-Mar-15 | Fluanxol 20mg | Left Arm |
| 18-Apr-15 | Fluanxol 20mg | Right Arm |
| 16-May-15 | Fluanxol 20mg | Left Arm |
| 13-Jun-15 | Fluanxol 20mg | Right Arm |
| 11-Jul-15 | Fluanxol 20mg | Left Arm |
| 08-Aug-15 | Fluanxol 20mg | Right Arm |
| 05-Sep-15 | Fluanxol 20mg | Left Arm |
| 03-Oct-15 | Fluanxol 20mg | Right Arm |
| 31-Oct-15 | Fluanxol 20mg | Left Arm |
| 28-Nov-15 | Fluanxol 20mg | Right Arm |
| 26-Dec-15 | Fluanxol 20mg | Left Arm |
| 23-Jan-16 | Fluanxol 20mg | Right Arm |
| 20-Feb-16 | Fluanxol 20mg | Left Arm |
| 19-Mar-16 | Fluanxol 20mg | Right Arm |
| 16-Apr-15 | Fluanxol 20mg | Left Arm |
| The following dates and links document when I was administered Risperdal Consta (a long-acting injectable). For context on the serious nature of this medication and its history, please see this link regarding Risperdal Settlements and Verdicts, which details several lawsuits against the manufacturer. | ||
| 30-Apr-16 | Risperdal Consta 25mg | Right Arm |
| 14-May-16 | Risperdal Consta 37.5mg | Left Arm |
| 28-May-16 | Risperdal Consta 37.5mg | Right Arm |
| 11-Jun-16 | Risperdal Consta 37.5mg | Left Arm |
| 25-Jun-16 | Risperdal Consta 37.5mg | Left Arm |
| 09-Jul-16 | Risperdal Consta 37.5mg | Right Arm |
| 23-Jul-16 | Risperdal Consta 37.5mg | Left Arm |
| 06-Aug-16 | Risperdal Consta 37.5mg | Right Arm |
| 20-Aug-16 | Risperdal Consta 37.5mg | Left Arm |
| 03-Sep-16 | Risperdal Consta 37.5mg | Right Arm |
| 17-Sep-16 | Risperdal Consta 37.5mg | Left Arm |
| 01-Oct-16 | Risperdal Consta 37.5mg | Right Arm |
| In a letter dated October 9, 2016, I informed psychiatrist David Cassar that I had never actually taken any of the pills he prescribed me prior to my 2014 arrest. This spanned the entire period from when he first began seeing me in 2002. Consequently, the conclusions reached by him and others in their court reports — which attributed my actions to "stopping the cure" (as I had led them to believe) — were entirely wrong. Instead of immediately informing the court that I had misled them, which resulted in their erroneous conclusions, he merely lowered the dosage slightly and abusively continued to experiment on me with injections and, later, pills. Most importantly, he kept me confined in a mental institution despite fully aware of my innocence. Do they really give you the option to refuse psychiatric medication, especially if it is making your life a misery? Of course not. To be a psychiatrist, one must seemingly be without a conscience, enjoying the destruction of what remains of their voiceless patients: their health — a precious asset that no amount of money can buy or restore once lost. In fact, the side effects of psychiatric drugs are so severe and dreadful that a psychiatrist's greatest satisfaction appears to be guessing which side effects will emerge, providing a further excuse to experiment on you under the guise of "combating" those very effects. It is a sadistic game. The only setback for these psychiatrists must be when their victims die earlier than expected (which, in cases like Mangion and Harrington, may have been the intention) or when a patient’s health becomes so ruined that further experimentation risks raising suspicion from relatives. In those cases, they simply move on to the next victim in the pipeline and start the process all over again. |
||
| 20-Oct-16 | Risperdal Consta 25mg | Left Arm |
| 03-Nov-16 | Risperdal Consta 25mg | Right Arm |
| 17-Nov-16 | Risperdal Consta 25mg | Left Arm |
| 01-Dec-16 | Risperdal Consta 25mg | Right Arm |
| 15-Dec-16 | Risperdal Consta 25mg | Left Arm |
| 29-Dec-16 | Risperdal Consta 25mg | Right Arm |
| 12-Jan-17 | Risperdal Consta 25mg | Left Arm |
| 26-Jan-17 | Risperdal Consta 25mg | Right Arm |
| 10-Feb-17 | Risperdal Consta 25mg | Left Arm |
| 24-Feb-17 | Risperdal Consta 25mg | Right Arm |
| 10-Mar-17 | Risperdal Consta 25mg | Left Arm |
| 24-Mar-17 | Risperdal Consta 25mg | Right Arm |
| 07-Apr-17 | Risperdal Consta 25mg | Left Arm |
| 21-Apr-17 | Risperdal Consta 25mg | Right Arm |
| 05-May-17 | Risperdal Consta 25mg | Left Arm |
| 19-May-17 | Risperdal Consta 25mg | Right Arm |
| 02-Jun-17 | Risperdal Consta 25mg | Left Arm |
| 16-Jun-17 | Risperdal Consta 25mg | Right Arm |
| 30-Jun-17 | Risperdal Consta 25mg | Left Arm |
| 14-Jul-17 | Risperdal Consta 25mg | Right Arm |
| 28-Jul-17 | Risperdal Consta 25mg | Left Arm |
| 11-Aug-17 | Risperdal Consta 25mg | Right Arm |
| 25-Aug-17 | Risperdal Consta 25mg | Left Arm |
| 08-Sep-17 | Risperdal Consta 25mg | Right Arm |
| 23-Sep-17 | Risperdal Consta 25mg | Left Arm |
| 08-Oct-17 | Risperdal Consta 25mg | Right Arm |
| 22-Oct-17 | Risperdal Consta 25mg | Right Arm |
| 05-Nov-17 | Risperdal Consta 25mg | Left Arm |
| 19-Nov-17 | Risperdal Consta 25mg | Right Arm |
| 3-Dec-17 | Risperdal Consta 25mg | Left Arm |
Every time you are injected with this diabolic poison, you feel humiliated and helpless. It feels like being forced into prostitution by a pimp (the psychiatrist) via a Treatment Order, or like a woman being raped for the umpteenth time, as your health is systematically ruined through the side effects of psychiatric medication just so the psychiatrist can earn a living and grow rich at your expense. You feel another part of your health slip away, watching your strength vanish bit by bit, yet you are powerless to stop it.
In total, I received 67 invasive treatments — 67 injections — for illnesses attributed to me without any scientific basis. These illnesses were intentionally invented by David Cassar, a fraudster of a psychiatrist who continued to drug me even after I told him that the conclusions in his court reports were based on my own false testimony, and that I had evidence to prove it. Is it not chilling? Are the words "sadist" and "tyrant" even enough to describe such evil? Was I not justified in previously describing psychiatrists as the incarnation of Satan on Earth?
Partners in Abuse: How Nursing Staff Perpetuate Psychiatric Malpractice and Sufferings While Remaining Silent Witnesses to Fraud
History shows that many Nazi leaders were found guilty of crimes against humanity and sentenced to death despite claiming they were "just obeying orders." If they were held accountable, why shouldn't the nurses and staff who administered these diabolical injections and pills be prosecuted? They made my life a living hell. Would I be excused for robbing a bank simply because my boss ordered me to do so, while I was fully aware a crime was being committed? It is even worse for these nurses; they are actively deteriorating a person's health, possibly leading to premature death. By doing so, they stain their hands with the crimes of psychiatry.
Psychiatrists can only inflict this much harm with the help of staff who cover up their abuses. These employees remain silent — and seemingly enjoy it — when a dosage is increased for no valid reason or to hide malpractice. The staff and nurses are 100% accomplices, working hand-in-hand with psychiatrists and protecting one another.
If someone were to infect a patient with AIDS using a contaminated needle, they would be prosecuted. Why, then, is someone excused for administering an injection they know will cause depression, parkinsonism, and other dreadful side effects? They cannot claim ignorance; even if they haven't experienced the effects themselves, every drug is supplied with a leaflet listing these devastating consequences.
It is a blatant case of "double standards" that proves a patient in a mental institution is stripped of all dignity. They might as well kill the patient — as likely happened with Mangion and Harrington — because it seems no one cares about their premature death, let alone prosecutes those responsible. Such deaths are often forged to appear as a "natural deterioration" of an invented illness, while those responsible are portrayed as dedicated staff who did their best. It is the same vile manipulation of facts that has allowed psychiatry to thrive for far too long.
Psychiatric Theater: A Cycle of Contradictions, Silencing Abuses, and Medication as a Tool for Submission
Seeing that he (Psychiatrist David Cassar) had failed to incapacitate me to the extent he desired through the use of Risperdal Consta — especially after I reported his numerous abuses to the Medical Council — he intended to subject me to yet another diabolical injection: Olanzapine / Zypadhera (see also: Zyprexa Lawsuit) . I was only saved when the authorities denied his request, likely due to the high cost. Instead, they began administering the equivalent pill, 5mg of Olanzapine daily, starting on December 17, 2017, as shown below.
The following images from my hospital file (click to enlarge) document the session on December 5, 2017, when Cassar arrived with the intention of drugging me with this injection simply because I had reported his abuses.



Transcript of Medical Records
(Note: Text in brackets [ ] reflects my own additions and translations):
Date: 5/12/17
Present: Patient seen with Dr. David Cassar
- Patient states (he is) feeling well. Claims his family has been informed of his situation.
- Feels he has spent enough time in hospital (3 years, 9 months).
- How do you feel about being sent to the hospital?
- States it might have been better to have been sent to prison, as he might have only served one year and "ma nkunx imcappas ghall-ghomri" [would not have been branded/locked up for life].
- Do you feel you needed to be sent here or needed admission?
- "Yes," he states he has accepted it. [Of course, because heaven forbid I dared state otherwise! It would be labeled "poor insight" and used as an excuse to drug me further.]
- But you have recently written to the Medical Council to the contrary. [This confirms, in black and white, that the Medical Council — instead of investigating my allegations of abuse — ignored me and covered for David Cassar. They even informed him of my complaint, allowing him to take revenge by further sedating and drugging me. They are wolves in sheep's clothing, doing the opposite of their duty at the taxpayers' expense.]
- Confirms this. Upset that he wrote to the Council for an investigation, but they instead informed Dr. Cassar of the complaint.
- Patient has written stating he believes he needs no treatment. [They were referring to the letter dated October 9 2016, which I sent to Cassar over a year prior, informing him that the court reports were based on wrong conclusions and that he must stop drugging me.]
- You are taking a small dose of injection.
- States that even if the dose is small, he experiences side effects; he only sleeps 2–3 hours, and his private parts do not function.
- Patient informed that for him to begin the discharge process, he would benefit from an injection depot. [While framed as a medical benefit, the requirement of a depot injection for my discharge was a coercive tactic. I was effectively threatened to accept the medication or remain detained indefinitely. It was a clear attempt to silence me, using the 'depot' to ensure I was subdued before I could ever be released. They essentially tell you that if you don't allow them to incapacitate you with say depression and Parkinsonism, they will make your life a hell to ensure you become depressed anyway — giving them a different excuse to drug you.]
- Patient states that he has always behaved himself and was appropriate in the ward, and that he had every right to write to the Medical Council regarding his situation.
- Patient reminded that Dr. Cassar "always tries to push him towards discharge." [This is another blatant lie. He claimed to be "pushing" for my discharge while vilely keeping me locked up and refusing to approve the leave I was entitled to — which had been approved by the Minister almost three months prior. He kept me innocently confined and drugged for over a year after I gave him that letter on October 9, 2016.]
- Informed patient that an application has been made for an Olanzapine depot (injection).
- This has not been approved yet.
- Patient is very worried about an increase in side effects, such as hypertension [one of its many side effects].
- Olanzapine tablets suggested [the equivalent of the Olanzapine depot].
- Patient refuses. He feels Dr. Cassar could be taking retaliatory action against him due to his complaints [referring to the reports I had made against him to the Medical Council and others].
- Does not wish to wait three hours once Olanzapine is taken. [Staff had previously briefed me that every time I received that diabolic Olanzapine injection, I would have to remain locked in the clinic due to the high risk of severe side effects. This is known as "Post-Injection Syndrome." A "syndrome" is a collection of signs characteristic of a disorder; in other words, after the injection, you are highly likely to suffer from a serious "disorder."]
- Dr. Cassar informed the patient that he does not want to give him anything that will increase side effects, but rather "medication which will help him." [I suggest you, the reader, return to this sentence after reading about "Post-Injection Syndrome" further below to see what David Cassar actually means by "help."]
- Wants to know what he is doing wrong: “Ghidli x’jien naghmel hazin. Qas li kont guinea pig, tlett injections differenti fi tliet snin u nofs.” ["Tell me what I am doing wrong. It's as if I am a guinea pig—three different injections in three and a half years."]
- The good points of changing the medication were explained to the patient. Dr. Cassar told the patient that from a clinical point of view, the patient is "not medically well" and there is "more ground to gain." [Note that according to him, I was "not medically well." He used this excuse to vindictively deny me the little leave I was entitled to. You have to be incredibly mentally strong not to fall into irreversible depression when dealing with such tyrants as Cassar and the Minister of Justice.
Continue reading to see the massive U-turn he was forced to make just a few days later, after I reported him again to the Medical Council and held them responsible for his vindictiveness. It was as if the Council told him: "Despite the fact that we are already risking too much to cover up your crimes, you have made Grech fully aware of our involvement to the point that he is holding us responsible for you denying him leave. Either give him his leave or we will have to proceed against you." My last email to the Medical Council was on January 15, 2018. Just four days later, on January 19, 2018 — as seen further below — Dr. Cassar arrived at MW3A all alone, without his usual "flock of sheep," specifically to approve the leave he had been denying me.] - “Ha taghmilli sarima ma halqi biex ma niktibx, Inti ghax qed nikteb qed taghmel hekk.” ["You are putting a muzzle on me so I won't write; you are doing this specifically because I am writing."]
- Patient advised that the depot [injection] he is currently taking can be stopped, and Olanzapine tablets begun, until the Olanzapine depot is approved.
- Offered to think about this.
- “Mela jien ghandi vuci, mhux li tiddecidi inti? Ghidli x’ghamilt hazin ha nitghallem. M’ghandix ghazla, xi tridni naghmel issa.” ["As if I had a say! Isn't it that whatever you decide happens? Tell me what I did wrong so I can learn from it. I have no choice; what do you want me to do now?"] — [Note how they so blatantly mock you by pretending to give you a choice when they had vilely decided long before which drugs to administer. In fact, it was written above that the "Olanzapine depot" "has not been approved yet" — proving they had a premeditated, diabolic plan regarding my medication long in advance.]
- Patient informed of the plan below and that, once Olanzapine is started, he will be reviewed for clinical improvement.
Plan:
Stop Risperdal Consta.
On the 17th, start Olanzapine 5mg tablets. [On December 17, I was supposed to receive another Risperdal Consta injection; instead, I was to begin taking this 5mg Olanzapine pill daily.]
In Summary:
- Recent writings to the media reflect his ongoing psychosis and total lack of insight.
- His repeated writings to the Medical Council reflect his ongoing psychosis with persecutory beliefs and a total lack of insight, including a firm belief that he requires no medication.
[Note that in the fraudulent field of psychiatry, simply stating that you do not need medication is viewed as a sign of mental health deterioration. Once you deal with psychiatry, you no longer have a voice; you become a nullity. You are forced to keep silent — a state termed "suffering in silence." You must remain quiet about the abuses you suffer, or else you will suffer even more. You become so discredited that speaking is not only useless but is used as evidence of "ongoing psychosis" or "persecutory beliefs." This is a dreadful reminder of the "delusions of persecution" label he used in my first court case to blatantly cover up the abuses of Magistrate Carol Peralta, who had threatened to smash me against a wall during a court sitting.] - His current dose of Risperdal Consta, which has had to be kept at a very low level due to side effects, is not controlling his condition.
[In other words, I was not sufficiently sedated or destroyed by medication to be silenced. By "controlling his condition," he really meant controlling me — preventing me from fighting for my rights and exposing the abuses I suffered. I had not yet been reduced to a complete imbecile. Abuses are so blatantly the norm in psychiatry that fighting them is viewed as an attack on the profession itself. It is a fake profession where the patient must be made voiceless at all costs, allowing them to experiment on victims with total leisure and liberty — especially when a patient attempts to expose the truth.] - He has repeatedly refused to change medication in spite of regular recommendations.
[As if I actually had a choice! Point 5 below contradicts this statement, proving they had already decided how to drug me long ago without any consultation. This is further confirmation that psychiatry is the art of blatant lies and the manipulation of facts.] - Olanzapine depot has not been approved by pharmaceutical services, and all applications for Olanzapine depot in the last four months have not been acceded to.
[Note the contradiction: if they claim in Point 4 that I refused to change medication, then who made the request for the Olanzapine depot? They are such blatant liars that they contradict themselves in almost every sentence. It is unbelievable that they made several applications within just four months. Despite being repeatedly refused, they kept trying, likely inventing new excuses to justify drugging me with this diabolic injection.
It is also worth noting that "four months" prior to December 5, 2017, would have been the end of July or beginning of August. This was only a month after I first wrote to the Medical Council (on July 6, 2017) regarding his abuses. He began his revenge immediately, aided by a Council that refused to investigate him. In Malta, one cannot expect authorities or investigative boards to be anything other than corrupt; they protect their own.] - I (Dr. Cassar) have also written to the Chairman and Chief Medical Officer about this in the past.
[It is abundantly clear that he even exerted external pressure to carry out his diabolical plan. His career was at stake, and he had to silence me before it was too late. By "Chairman," he is likely referring to his close friend, the Chairman of Psychiatry, Anton Grech. I had informed Grech of Cassar’s abuses in a letter dated October 26, 2016, but he chose to cover for his colleague by doing nothing. Instead of investigating, he vilely reported my complaints back to Cassar.] - He has now finally accepted to switch treatment to Olanzapine, and this will be converted to depot treatment when finally available.
[This is yet another blatant lie. I certainly did not "accept" to switch to such a diabolic injection; after all, did they not claim in Point 2 that I had a "firm belief that he requires no medication"? I was not consulted; I was vilely forced. This was imposed on me without any choice, as if I were an animal. In psychiatry, the patient is not considered human but is reduced to a mere guinea pig.
Ask yourself: if he started in Point 1 by discrediting me as someone with a "total lack of insight," how can he then contradict himself by claiming to consult me — someone he views as an imbecile with "ongoing psychosis" — about my treatment? He is a blatant liar. Because he had a Treatment Order imposed on me since my first court case, he had the liberty to drug me however and whenever he liked. I had absolutely no say. As a psychiatrist, he is such a practiced liar that he cannot help but contradict his own written statements.] - Olanzapine oro-dispersible will be started with close supervision of ingestion by nursing staff.
[Note again the self-contradiction. Earlier, he portrayed the situation as if he were discussing medication options with me. In this sentence, however, he is not only imposing a drug he chose himself but is also ordering the staff to maintain "close supervision" to ensure I ingest it.] - It has to be noted that he has repeatedly stated that when on oral medication he reported taking it, but never did.
[Here, he is again referring to the letter dated October 9, 2016, which I sent him over a year prior. He is confirming that he was fully aware that the conclusions he and others reached in their court reports were totally wrong. He and the other "experts" fell for my bait completely. But in psychiatry, facts and truth do not matter; only blatant lies and the manipulation of facts prevail. From a field that fake, one should expect nothing but fraudulent and incorrect conclusions.]
Signed:
Dr. E. Camilleri on behalf of Dr. Cassar [This E. Camilleri was likely a recent graduate in psychiatry, simply parrot-writing what her mentor, Cassar, dictated.]
Dr. David Cassar, Reg. No. 1674
Date: 19/1/18
Location: At Ward
- No prominent changes in behavior.
- Has been compliant with treatment.
- Remains with very poor insight.
- In view of compliance with oral Olanzapine and with a view to converting to long-acting Olanzapine when available.
- Plan:
— To start 4 hours per week leave, accompanied at all times by relatives.
— Relatives to sign awareness that he needs to be accompanied at all times.
Signed: Dr. D. Cassar, Reg No. 1674
[Note that for this session on January 19, 2018, the handwriting is Cassar’s own. This time, instead of bringing his usual "flock of sheep" and a junior doctor to transcribe his dictation, he came entirely alone. It was as if he felt too ashamed to swallow his own words and approve the leave in front of his subordinates—leave that he had been vindictively denying me for months. He was forced into this complete U-turn just a few weeks after claiming I was getting worse. According to his own notes, I still "remained with very poor insight," yet he suddenly granted the leave he had previously blocked. This change only happened because I had emailed the Medical Council on December 7, 2017, and January 15, 2018, holding them responsible for his tyranny.]
Date: 14/2/18
Location: Ward Round
- Present: Dr. Bezzina Xuereb [For more information on Psychiatrist Maria Bezzina Xuereb and how she vilely overdoses patients to cover up staff abuses — as she did in my case — see further below].
- Patient requesting more leave: currently on 4 hours once a week; wishes to increase leave to 5 hours twice a week, as per the Minister's approval.
- Plan: To discuss with Dr. Cassar.
If you think calling the Olanzapine injection (Zypadhera) 'diabolic' is an exaggeration, consider the image below regarding its frightening Post-Injection Syndrome (available via [this link] or [this website]). This syndrome involves side effects so severe that patients must remain in the clinic under continuous monitoring by a staff member for no less than three hours after every dose.

MENTAL HEALTH SERVICES (this is some other name given to this so fake mental institution / hospital)
MONITORING CHART FOR SERVICE USERS ON ZYPADHERA LONG ACTING INJECTION
Post Injection Syndrome:
- Usually occurs within three hours of Zypadhera depot.
- Needs urgent medical attention.
- Symptoms are: sedation and delirium (disorientation, confusion, agitation, anxiety and other cognitive impairment).
- Symptoms also include: extrapyramidal symptoms, dysarthria (slurred speech), ataxia (staggering, uneven gait), aggression, dizziness, weakness, hypertension and convulsion.
- The three hour observation period should be extended as clinically appropriate for service users who exhibit any signs or symptoms consistent with Zypadhera overdose.
Date & Time: Temp. __, Pulse __, Resp. __, Blood __, Pressure __
Allocated Member of Staff
Observations:
- Is the service user alert and mobilising?
- Is there any evidence of sedation or delirium?
The dreadful Post-Injection Syndrome associated with the diabolic injection Olanzapine (Zypadhera) is a perfect example of what the ancient Romans called 'RES AUDITU CRUDELIS, VISU NEFARIA'—a thing cruel to hear and evil to see. If only they knew that centuries later, such horrors have become the routine norm in the 'fake' branch of medicine known as Psychiatry.
We are living in an unfortunate era where many remain silent as to how Psychiatry is vilely used to experiment on victims in such a humiliating, inhumane, and sadistic way. It is equally vile that they list the dreadful side effects they expect you to suffer, yet offer no remedies to alleviate them. Are they merely interested in how high they can drive your pulse? One must wonder how such drugs ever met the 'benefits outweigh the risks' requirement for approval. It seems that as long as the risks aren't immediately lethal, the industry finds it acceptable to make a patient’s life miserable and ultimately shorten their lifespan.
If standards were higher, Psychiatry’s true face would have been exposed long ago; but in a 'big business' world, money speaks and silences opposition. This glimpse into Post-Injection Syndrome clarifies what Psychiatrist David Cassar truly meant by 'medication which will help him.' If a drug causes such immediate dread, one can only expect the long-term 'help' to result in complete disability. In Psychiatry, everything has the opposite meaning: 'to help' actually means to destroy, sedate, and reduce a human being to a physical and mental wreck.
We condemn the Nazis for human experimentation during war, yet we allow Psychiatrists to perform even more dreadful experiments on vulnerable patients in times of peace, all under the guise of 'curing' them.

My treatment with Olanzapine started on December 17, 2017. I was given pills because the injection was not approved — not because authorities were worried about its horrific side effects, but most probably because the depot form was too expensive. To them, it was a matter of cost, not patient safety.

Regarding point 4 above, where Psychiatrist David Cassar claims that I “repeatedly refused to change medication,” this is a blatant falsehood. In reality, I never had a say in my treatment because a Treatment Order was enforced upon me by Dr. Cassar himself during my first court case.
The forced "consent" to being treated as a "guinea pig"
Furthermore, the following image demonstrates that I lacked any agency due to a "consent form" I was forced to sign. This document effectively granted them permanent approval to medicate me at their discretion. In practice, this "forced consent" is an admission to being treated as a "guinea pig," allowing psychiatrists to override a patient’s will.
It is important to note that if the authorities intend to impose a Treatment Order, they will find a way to do so regardless of the patient's wishes, rendering the concept of "consent" meaningless. It functions much like a "show trial," where a fair hearing is promised, but the sentence has already been determined by the police and the media before the proceedings even begin. As a friend once observed, the court often delivers the sentence that the majority desires; meanwhile, the elite are excused and their actions justified through a different set of rules.

English Translation
Ministry for Health: Mental Health Services
Informed Patient Consent for Treatment
Treatment for: (Insert Diagnoses)
— Asperger’s Syndrome
— Depression (?), CCJP
Expected Benefits:
— Alleviation of symptoms / Management of illness
Declaration by Patient
— The treatment has been explained to me, and I have been informed of the purpose and expected benefits, as well as the potential risks if this treatment is not administered. Where relevant, I was informed of alternative treatments.
— I have also been informed of the potential risks associated with receiving this treatment.
— (Unmarked) I waive my right to be provided with information regarding the benefits and risks of this treatment.
— I understand that the results of this treatment cannot be guaranteed.
— I was given the opportunity to ask questions and discuss my concerns.
— I give my consent to undergo the treatment as it was explained to me.
— I understand that I have the right to change my mind and refuse the proposed treatment at any time, provided I inform my doctor.
Declaration of the Physician Obtaining Consent
— (Unmarked) I have explained and discussed the proposed treatment with the patient, including the benefits and the risks (both general and specific) pertaining to them.
— (Unmarked) I provided the patient the opportunity to ask questions, which I have answered to the best of my knowledge.
Date: 15-Jun-14
Name and Surname: Maria Axiak, Reg. No. 2727,
Position: Consultant
Analysis:
This "consent" document was distributed to patients, including myself, at the Forensic Ward of Mount Carmel Hospital on or around 15 June 2014. The form was handed to me by a nurse who filled out the basic sections; the rest was completed by Psychiatrist Maria Axiak. Dr. Axiak used almost illegible handwriting, seemingly to avoid accountability for listing my diagnoses as Asperger’s Syndrome and Depression.
The dishonesty here is blatant. First, Asperger’s Syndrome had never been mentioned to me before, and it is a condition for which there is no "cure" — rendering this "consent for a cure" logically meaningless. Second, regarding the depression diagnosis: it appears she intended to manufacture this condition by drugging me with Risperdal from the moment I was admitted to the Forensic Ward in 2014. They essentially created the symptoms of depression and then used those symptoms as a pretext to force further treatment upon me. When dealing with a psychiatrist, one must look past the professional mask to decipher their true intentions.
The final point of the patient declaration — stating that I have the "right to change my mind and refuse the proposed treatment at any time" — is nothing more than a "sugar-coated pill." As my hospital file transcripts confirm, I never possessed such a right.
Furthermore, had I refused to sign this form, it would have been weaponized against me. Because my second court case was already prejudiced by the assumption that I was mentally ill, a refusal to sign would have been interpreted as an intent to stop medication. This, in turn, would have been used as a justification to keep me detained indefinitely. This is "indirect consent" by coercion. As my hospital file explicitly states: “Patient informed that for him to begin discharge process he would benefit from injection depot.” This proves the "consent" was fake; the treatment was a requirement for my freedom.
Regarding the "Expected Benefits" listed as "Alleviation of Illness," it seems that intentionally inducing depression and Parkinsonism through Risperdal was their version of "alleviation." They manipulate facts to frame their harm as a "benefit." Their ultimate solution for controlling behavior is to disable the individual. Much like stopping a thief by cutting off their hands or a rapist by castration, they attack the mind. By disabling a person’s mental capacity, they strip away the ability to fight for one's rights, reducing the patient to a state that serves as an excuse for further over-medication.
The Systemic Abuse of Power
With the psychiatric system being as inherently abusive as it is, one can never truly be prepared for the extent of their mistreatment. While many cases follow a predictable pattern of repetition, even the most sophisticated risk assessments cannot predict the level of calculated sadism these individuals are capable of. The following incident illustrates this point clearly.
On 4 April 2018, a nursing aide refused to give me my usual morning yogurt and egg — presumably so more would remain for the staff to take for themselves later. Later that day, upon returning from a few hours of home leave, I brought a camera back with me.
When the evening meals were distributed, I observed the same nursing aide beginning to collect the numerous leftovers to take home. I approached with my camera to photograph him in the act, intending to secure proof of this theft and, by extension, incriminate the rest of the staff who had long turned a blind eye to such corruption.
What happened next was truly incredible:

Incident Details
Date: 4/4/18
Reporting person's name: Victor Gelfo, Grade: Senior Nurse
Witness/es names: Patrick Farrugia, Grade: Senior Nurse
Details of Incident/ Accident: Patient was taking photos of food in tray, claiming that food is stolen.
Reported to: Senior Nursing Officer, Consultant.

Medical description of Incident/ Accident: Escalation of behaviour with inappropriateness secondary to inappropriate beliefs as identified in patient's file.
Clinical management of Incident/ Accident: Well-documented in patient's file and nursing report.
Follow up: Plan as per file
As for Nicole Sciberras, she was most likely a recent psychiatry graduate, simply acting like a parrot and writing down whatever they dictated to her.

Actions taken - Immediate: Patient told that he is not allowed to take photos in hospital grounds. Camera taken from him.
Actions taken - Long term: Patient was reviewed the next day by Dr. Maria Bezzina Xuereb. The Consultant was informed and TREATMENT ADJUSTED.
The Suppression of Evidence and the "Illusion" Narrative
It is worth noting the phrase, "Camera taken from him." They confiscated the camera specifically to delete the evidence that would have incriminated them. This allowed them to reframe their own misconduct as my "illusions" — a form of "crime-laundering" typical of the psychiatric system. My legitimate observations were then labeled as "inappropriateness secondary to inappropriate beliefs," creating a false pretext to have me further drugged and sedated.
This pattern mirrors the actions of Cassar and Peralta in 2002, when they confined me to Male Ward 10 at Mount Carmel Hospital. Their goal was to discredit me and carry out a character assassination by labeling me "mentally ill." Cassar vilely portrayed the actual abuses I suffered as "delusions of persecution." In the realm of fraudulent psychiatry, the story is almost always the same: a blatant manipulation of facts supported by outright lies. The victim is victimized repeatedly, while the abusers not only escape accountability but use their power to retaliate, forcing the victim to "learn the lesson" through savage and systemic abuse.

And voilà! Just like that, the dosage was vilely doubled on April 6, 2018—increasing from 5mg to 10mg. That is an impressive 100% increase. Note how I was prescribed this pill at twice the original dosage with instructions to "always dissolve in a glass of water." Because it was an "orodispersible" tablet — designed to dissolve instantly upon contact with water or saliva — the psychiatrist could ensure I was taking it. This guaranteed I would suffer the intended, diabolic side effects and sedation even more.
(Look again at the consent form above and ask yourself how blatantly they lie to and deride you. It claimed, "I understand that I have the right to change my mind..." — yet I clearly never had that right.)
Even if doubling the dosage didn't achieve its full intended effect, the underlying goal was to remind me that I am a voiceless guinea pig in their hands. It serves as a warning: whatever abuses you dare expose, you are no match for them. You will pay a high price with your own health. Next time, the side effects might be urinary incontinence; then, they might make you sick with diabetes, and so on.
Since psychiatry is built on the art of the blatant lie, they fell back on the usual fabrication, claiming I held "inappropriate beliefs." Yet, they managed to contradict themselves in the same incident report, writing that the dosage increase was actually because the patient "is not allowed to take photos on hospital grounds" (apparently, privacy is only an exceptional concern for the exceptionally corrupt).
By their own sadistic logic, doubling the dosage is meant to prevent the victim from ever again having the physical or mental ability to "take photos" that might incriminate them. In other words, these diabolic psychiatric drugs "solve" your "inappropriate beliefs" by disabling you, destroying you, and ultimately killing you prematurely — just as they did to Mangion and Harrington — after you have spent your final years reduced to a state of total disability.
In reality, while one is not allowed to take photos of patients, this rule is weaponized to hide vile abuses by staff — such as employees taking home food intended for patients to feed themselves and their animals. Allowing this leads to a cycle of abuse where staff intentionally used to order more food than necessary so there was a "surplus" for them to feast on.
It is no mystery why many nurses in this hospital are so significantly overweight; they blatantly feast on patient rations. During night shifts, with the patients drugged and sedated, they have almost nothing to do but sleep. Psychiatry is a rewarding career for them in that sense. Why single out someone like Theuma for being paid for three months without showing up, while ignoring these blatant thieves who show up for the night shift only to sleep, and the day shift only to steal food and play on their mobiles?
As for the term "inappropriate beliefs," it is merely a psychiatric euphemism for hallucinations or symptoms of schizophrenia. It is a tool used by the "art of psychiatry" to discredit a victim's testimony — reframing hard facts as mere imagination or illusions.
Psychiatrist Maria Bezzina Xuereb clearly learned well from her mentor, David Cassar, who vilely abuses his victims. Much like a fortune teller pretends to see the future to fool you, a psychiatrist pretends they can cure you. Yet, they cannot even perform a brain scan to prove a diagnosis like schizophrenia. Everything is based on presumptions and blatant lies rather than clinical facts. You cannot expect anything better from a field that is fundamentally fake.
In the months prior, while I was still being administered the diabolic Risperdal Consta injection, I repeatedly asked Dr. Xuereb during her fortnightly ward rounds to lower the dosage because of the dreadful side effects. She always offered the same excuse: that I was already on the minimum dose. Her theory was that "as time passes, the body becomes accustomed to the medicine and requires an increase in dosage rather than a reduction." In simpler words: this "fake" science only makes you sicker, requiring constant increases in dosage over time. When dealing with something fraudulent, you can only be ruined; it may appear to treat one symptom while destroying you in a multitude of other ways.
Regarding this incident, I asked her in vain to review the camera evidence and involve the police. But in psychiatry, evidence and facts are ignored in favor of cover-ups, lies, and the manipulation of truth. Being a fraud herself, she ensured the evidence was destroyed beyond recovery. I was drugged further in the hope that I would be too disabled to report these abuses — specifically her criminal act of covering up those involved.
Finally, the note stating "the Consultant was informed" confirms that David Cassar had full knowledge of these events. Once again, he sided with those abusing their positions — covering for staff stealing food by maliciously attributing "inappropriate beliefs" to me. It is truly a case of old habits dying hard.
This time, Cassar had the full support of the staff to vilely overdose me by doubling my dosage. Previously, staff had reported that I always behaved well, which deprived him of the excuse he needed to drug me further.
I reported him to the then-Commissioner for Mental Health, John Cachia, the following day on April 6, 2018. Initially, he ignored me, callously failing to reply to my email. It was only when I wrote again nearly two weeks later on April 19, 2018, threatening to involve the media, that he finally acted. However, he merely sent two "puppets" from his office — Psychiatrist Joe Saliba and a certain Dr. Noel Vella — to perform a superficial cover-up under the guise of an investigation. They, predictably, found nothing wrong.
If Cachia were serious, he would have acted immediately upon my first email rather than waiting until I issued a threat. If the police were serious about a report of a teacher molesting a student, would they wait days to act? Would they give the teacher time to take revenge, corrupt witnesses, and destroy evidence?
Naturally, these investigators were prejudiced against me, a mere patient. In their world, one doctor never contradicts another. Especially in psychiatry, the patient is always to blame, and no opportunity is lost to conduct vile experiments on them. Of course, no action was ever taken against the staff. They are trained to see the speck in the patient’s eye while ignoring the massive log in the eyes of the staff and their fellow doctors. In other words, they are built for corruption: to maliciously shield the abusers and cast blame upon the victims.
Regarding the nurses involved: the one listed as a witness, Patrick Farrugia (whom I mentioned in a previous incident without naming him), was the person who, in a fit of rage, threw away my evening meal on April 4, 2018. As for Victor Gelfo, the one filing the report, one can gain a clearer understanding of his character from his Facebook page, shown below:

As shown, Victor Gelfo superimposed onto his image the symbols of a certain "religion of peace" — a religion inspired by a man who, in his 50s, married a six-year-old girl and consummated the marriage when she was nine. In his Facebook post, Gelfo calls a priest from Mosta a "hate-monger" and questions why the police have not acted. I hope he won't mind if, one day, the police investigate him for standing by while I was vilely drugged and overdosed. He witnessed a 100% dosage increase intended solely to silence me for uncovering staff abuses — abuses he was fully aware of and should have reported himself. Instead, he did the unthinkable and reported me. It is like reporting a teacher’s abuse only to find the "cannons" pointed at the victim, who is then labeled "mental" to discredit them while their evidence is destroyed.
To illustrate Gelfo’s character: he was the type who often "trusted" patients by handing us the keys to open the ward door ourselves — for instance, to go to the Main Garden — expecting us to lock up and return the keys. However, one day he handed the key to a patient, MC, whose leave permissions had been revoked because alcohol was found in his blood. This patient promised to return by 16:00, which he did.
But when Gelfo realized he shouldn't have let him out, he scrambled to cover his tracks. He called the doctor and fabricated a story, claiming the patient had pushed a foreign carer and "escaped" by running away. This patient was diabetic and so overweight that he could have never walked away quickly, let alone "run" or "escape" without being caught within half a meter. (Rest assured, they would have knocked him to the ground even more savagely than they did the young "giant" mentioned earlier).
Predictably, the psychiatrist — the usual fraud — blindly believed Gelfo’s version without even considering the patient's side. The patient was eventually sent to another ward for several days as punishment; I only hope he wasn't overdosed as well. This is another example of how fake psychiatry is: it is based solely on blatant lies and the manipulation of facts. They are always prejudiced against patients, viewing us as imbeciles or guinea pigs to be abused and drugged at will.
In Gelfo's case, his own incompetence (being "fooled" into giving a key to an unauthorized patient) was maliciously reframed as the patient "intentionally abusing" the "dedicated" staff to escape.
But then again — in this system — who bloody cares?

The above is a "Record (of) patient's valuables," documenting when my Fujifilm camera was taken into the hospital’s safe on April 5, 2018. It was only returned to me nearly two months later, on May 31, 2018. Instead of forwarding the device to the police to recover the photos and evidence within, they ensured that the evidence was destroyed forever, leaving no chance for them to be incriminated. Such is life in a mental institution: the staff are the culprits — always excused and protected — while the patients are the victims, yet always the ones to blame.

Just as a fortune teller makes a fortune by defrauding clients — pretending to predict their futures — psychiatry is a fraudulent business operating on a far vaster scale. In fact, despite continuous advancements in medicine, science, and technology, there is a total lack of progress in psychiatry.
Instead, the field moves in the opposite direction; the number of people diagnosed with mental illnesses is maliciously and fraudulently increasing. Previously, they claimed these illnesses affected 20% of the population, then 25%, and soon they will likely claim 33%. In corrupt Malta, psychiatrists have already inflated this figure to an incredible 66%! (See the video above, downloaded from none other than Malta’s national broadcaster, Television Malta).

In the thought-provoking article "The Lie of Mental Illness," it is noted that people no longer simply feel "sad" or "depressed" — now, they are all labeled "mentally ill" or "bipolar." In the world of psychiatry, if you mention a hobby like cycling or historical research, you risk being labeled as "obsessive." Conversely, if you say you have no hobbies, you face the same risk; they will claim you became depressed because you lacked a pastime.
Psychiatry is a vicious cycle: the more people are intentionally and falsely diagnosed, the greater the demand for psychiatric drugs, directly benefiting pharmaceutical firms. Through their dreadful side effects — which can reduce patients to a state of disability or induce deeper depression — more people are forced to seek further psychiatric "services." This maximizes profits for both parties, as they work hand in hand.
The Guardian article, "Profiting from mental ill-health," offers further insight with the phrase: “There's a reason psychiatrists prescribe drugs rather than talking therapy: the latter makes no money for pharmaceutical firms.” Later, the same article asks: “Do these psychopharmaceuticals work to restore mental health? Actually, the evidence is overwhelming that they fail.”
This brings us back to the ancient Roman proverb: "CUPIDITAS RADIX OMNIUM MALORUM," / "Greed is the root of all evil." To illustrate what I mean by this insatiable greed — and the resulting insatiable evil — let us examine the following image.
Conflict of Interest, Misconduct, Use of Public Resources

The above screenshot displays the "Clinical Services" at Mount Carmel Hospital as of 2020. It lists eleven clinical firms and the psychiatrists purportedly assigned to them on a full-time basis. While these consultants are salaried for full-time positions, I contend that their actual hours worked tell a significantly different story.
Specific Observations on Clinical Staff:
- Dr. Maria Axiak: Listed under "General Psychiatry, Old Age, and Forensic Psychiatry." My first encounter with her was in 2014 during my second court case while I was held in the Forensic Ward. This is the same ward where the previously mentioned patients, Mangion and Harrington, passed away in their 50s displaying symptoms typically associated with "Old Age."
- Dr. Joseph R. Saliba: Listed under "General Psychiatry, Child & Adolescent Psychiatry." In 2018, Dr. Saliba was dispatched by then-Commissioner for Mental Health, John Cachia, to investigate my case. Rather than investigating the staff abuses I reported, he facilitated a cover-up, resulting in Dr. Cassar doubling my dosage of Olanzapine. Dr. Saliba’s name also appears in my 2002 court records; although he was appointed by Magistrate Carol Peralta to assess me, he later renounced the role.
- Dr. Ethel Felice: Listed under "Perinatal Psychiatry." She was involved in the report for my second court case. It appears she acted largely as a "rubber stamp" for the two dominant male psychiatrists who have been involved in my case since 2001, failing to question their findings.
- Dr. David Cassar & Dr. Anton Grech: Dr. Cassar is listed under "Community Services and Rehabilitation," while Dr. Grech is listed as the "Chairman of Psychiatry." I have observed Dr. Cassar conducting ward rounds accompanied by a large group of students or junior doctors, possibly receiving additional allowances for this "expertise."
{kind=link}
Many of these psychiatrists frequently appear on television programs. While these appearances may not be directly remunerated, they serve as a powerful marketing tool to drive patients to their private practices.
It is common for these consultants to augment their government salaries with highly profitable private clinics, often charging upwards of €50 per consultation. There are serious questions regarding whether this private income is fully declared for tax purposes. Furthermore, there is a blatant conflict of interest: one can simply email a consultant at their official hospital address to inquire about their private services, and they will readily provide the details without any apparent ethical hesitation.
The gravity of the situation is best illustrated by the blatant overlap between public duties and private gain. It is common practice for these psychiatrists to use their government email addresses to conduct private business. Furthermore, when appearing on television to share their opinions, some have been known to provide their private clinic details to callers on air.
There is a pervasive culture where patients in the public sector are subtly — or explicitly — encouraged to seek private consultations to "jump the queue." The prevailing attitude seems to be, “Ta' b'xejn, servizz ta' b'xejn tieħu” (You get what you pay for with a free service). I am specifically referring to the conduct of individuals such as Anton Grech, David Cassar and Hector Cutajar, who utilize their public offices as marketing platforms for their private practices.
In addition to their salaries, many of these individuals receive extra allowances as court-appointed experts where, from my experience, they just provide reports filled with presumptions and blatant lies. Their erroneous conclusions serve to condemn innocent individuals to mental institutions, effectively facilitating "medical experiments" or covering up systemic abuses.
Dr. Hector Cutajar further supplements his income by serving on Medical Boards. I vividly recall my appearance before such a board on Monday, 14 December 2015. Upon seeing me, Dr. Cutajar remarked to the other members, “This is a true case; I know him and his case well. He is schizophrenic with severe obsessive disorder.” This bias was so influential that another board member, seemingly forgetting her role was to investigate sick leave abuse, asked if I had ever worked in my life ("Ġieli ħdimt qabel?"). This was an incredible insult, considering that prior to my 2014 arrest, I had worked for 15.5 years without taking a single day of sick leave — with the exception of the 37 days I was maliciously detained by David Cassar. Ironically, due to the interventions of the psychiatric system, my record has now shifted to the opposite extreme.
Academic Roles and Excessive Appointments
Greed and the pursuit of influence seem to drive these individuals to take on even more roles. Many serve as lecturers, "indoctrinating" the next generation of doctors. In a system as compromised as Malta’s, it is no surprise to find Dr. David Cassar serving not only as a Senior Lecturer but also as the Head of the Department of Psychiatry at the University of Malta.
It is difficult to decipher which role was actually his "full-time" commitment — Consultant Psychiatrist at Mount Carmel Hospital, Head of Department at the University, or a combination of both — alongside his private practice and court duties.

The list of visiting academics within the University of Malta’s Department of Psychiatry — during David Cassar’s tenure as Head — included the previously mentioned Ethel Felice and Cassar's cousin, Joseph Cassar (whose names I have not highlighted). Notably, Joseph Cassar may not have worked at Mount Carmel Hospital during his time as a Minister, but he resurfaced there later. (He possibly secured his position through other means, ultimately leading to his resignation from Parliament despite playing it the victim). Also listed are Maria Axiak and Maria Bezzina Xuereb, both of whom I have mentioned before.
Though I cannot confirm this with 100% certainty, I was informed that while the PN was in government (in the years preceding the 2013 election), David Cassar was appointed Head of Psychiatry at Mater Dei Hospital while his cousin, Joseph Cassar, served as the Minister of Health under the Gonzi administration. During this period, David was rarely seen at Mount Carmel; however, his presence was felt once again after he was removed from that post following the 2013 change in government.
In the same way the incoming 2013 Labour Government signaled its corruption by placing Super One staff on the state payroll, I suspect that many of David Cassar’s colleagues — including Joseph R. Saliba and Roberta Holland — secured their roles as visiting lecturers at the University on similar grounds. I also suspect a "power exchange" between David Cassar and Anton Grech: one is a Head at the University but leads a firm at Mount Carmel, while the other is Chairman of Psychiatry at Mount Carmel but serves as a visiting academic at the University (where lecturers reportedly earn over €80 per hour).
Furthermore, the Doreen Cassar highlighted in the list is none other than David Cassar’s wife — a blatant case of nepotism. She also received an allowance as a ymember of the Medical Council, where she likely used her position to further cover up her husband’s crimes and abuses against me.
Driven by an insatiable greed for multiple income streams, I doubt these individuals have any time left for family or normal pastimes — assuming their full-time jobs consist of 40-hour weeks like us "normal mortals." Perhaps their "sadistic" pastime of drugging and ruining their victims' lives — while being paid to do so — more than compensates for the lack of a personal life. To complete the circle, our "noble" University also utilizes the services of the former Commissioner for Mental Health, John Cachia.
If you want to sum up what the University of a typically corrupt country like Malta represents, look no further than the "illustrious" Andrew Azzopardi. Years ago, he published an article about my case titled, “... Ran out of dogs? A sick mind on the rampage.”
Thank God that I — the one he labeled a “sick mind” — was merely using dark humor regarding dead animals I found while cycling, animals already killed by irresponsible drivers. God forbid I were a true, unscrupulous sadist like him. Instead of dealing with animals already found dead< in abundance, he enjoys “crucifying” innocent human beings without checking the facts — as seen in his earlier article, “Crucify him - Crucify him!”
What is truly impressive is that despite this behavior, he was not only made a Professor but also the Dean of — wait for it — the Faculty for Social Wellbeing at the University of Malta. Perhaps the next step is for our corrupt state to award him the Ġieħ ir-Repubblika. To earn it, he’ll likely just need to introduce a new course on the most efficient way to crucify the innocent.
With the departments of Psychology and Criminology under his wing, and people like Roberta Holland listed as senior lecturers, I am convinced they will succeed in indoctrinating the next generation. Under the guidance of those who so easily brand others as "mentally ill" or fit for "crucifixion," the future of "Social Wellbeing" in this country looks increasingly sadistic.
Sleeping on the Job, Stealing the Food: A Nurse’s Guide to Mount Carmel
The video above is one I am convinced you will find interesting. It reveals a typical night in the "fake" mental institution of Mount Carmel Hospital. Here, many of the staff do their utmost to make the lives of patients even more miserable — such as forcing patients to go to bed early simply because the staff want to sleep themselves.
They get away with it because their superiors — the doctors and psychiatrists — are even worse. The vulnerable patients under their care are so voiceless and stripped of dignity that if they dare report these abuses, they risk being labeled with "inappropriate beliefs." This becomes an excuse to drug them further, as happened to me and as outlined in the cases below.
I intentionally uploaded this video from a night when one particularly pathetic nurse was in charge of the Halfway House. While the others weren't much better, he stooped to especially low levels. Normally, he would sleep from 10:00 p.m. until after 5:00 a.m., despite only being allowed a two-hour break.
Notice how the clinic remained closed while the ten female patients were locked behind the "Female Side" door, with the female nurse asleep in her own room. When the original FW3A ward was split to create the HWH, the corrupt hospital administration actually spent money to build the staff a room large enough for a bed, shower, and toilet — an "en suite" for their comfort! Rest assured, they didn't lock those doors to prevent patients from having sex; most were already rendered sterile by psychiatric drugs (if anyone even cares).
Adjacent to the air-conditioned Male Staff Room — where this nurse slept in total darkness with the door chained slightly ajar — was the patients' bathroom. It contained two toilets and two showers, but he kept it locked all night so no one woke him up by flushing or showering. Consequently, the ten male patients were forced to share a single toilet located near the dormitories. To avoid waking each other up, we often didn't flush, meaning we paid the price with a sickening stench by morning.
Some patients were so heavily sedated with drugs and injections that they ended up urinating on the floor. Others, finding the single available toilet occupied and unable to hold it any longer, were forced to do the same. This led to a desperate situation where someone might have to take the sheet from their own bed and lay it on the floor just to absorb the urine and keep their shoes dry.
The only alternatives were to stop drinking hours before the forced 10:00 p.m. bedtime or to keep a cup or plastic bottle by the bed to pee in instead. We were forced into the habits of "primitive cannibals" just to avoid stepping in waste at the only toilet left open to us.
In contrast, the female patients had three toilets separated from their rooms by a corridor. The female nurse had her own private "en suite" shower and toilet, plus another one available in the clinic. Similarly, the male nurse had access to the clinic toilet as well as the two patient toilets located right next to the room where he slept.
To make matters even more vile, when he finally opened those two patient toilets in the morning, they were often stained with his own urine. Being too lazy to walk to the clinic, he likely used them while half-asleep. If these two toilets had been left open for the ten male patients during the night, we would have had three toilets at our disposal —bjust like the women — and a better chance of finding one that wasn't filthy.
In summary, during the night shift, the male nurse had three toilets to choose from (a 1:3 ratio), the female nurse had two (1:2), the ten female patients had three (10:3), and the ten male patients were left with just one (10:1). It is impossible not to curse your luck ending up as a patient in this "hospital," where you were treated like an animal so that staff could abuse their positions and collect a salary while sleeping the night away. (And again, why blame someone like Theuma when this has been the culture since time immemorial?)
Note how, once that pathetic male nurse woke up sometime after 5:00 a.m. and opened the male toilets, then later woke the female nurse at 5:30 a.m. Incredibly, she then relocked the "Female Side" partition door, leaving the ten female patients locked away alone until 6:00 a.m. (Truly incredible — it’s like leaving a child locked in a room with two Great Danes). Meanwhile, she (seen in the video at 9:07) was feasting in the staff pantry, eating and drinking until she became even more bloated. The male nurse had done the same before her, helping himself to the ham and cheese sandwiches intended for the patients later that day.
Notice at the 9:00 mark of the video that the kettles were still empty and upside down. This nurse was so lazy that he found it too much trouble even to provide us with four tablespoons of coffee; he left the simple task of boiling water to the responsible carer instead.
During the day, except for two hours after dinner, some staff had the sadistic habit of closing the female partition and the male dormitories. This was done to prevent patients from sleeping during the day, under the excuse that they wouldn't sleep at night (which, indirectly, would prevent the staff from sleeping through their own night shifts). Of course, if a patient struggled to sleep, there was always an injection of Ativan or Valium to sedate them so heavily that they would end up wetting themselves in bed by morning.
In these instances, the twenty male and female patients had only the two "Male" toilets near the staff room at their disposal (a 10:1 ratio) instead of the six toilets (a 3.3:1 ratio) that should have been available.
Toward the end of the video, you can see that the male and female staff rooms were equipped with beds, along with a spare bed in the clinic. In the footage of the female staff room, you can see sofas, furniture, and numerous sanitizers — used as if the staff feared catching leprosy from the patients they considered scum. You can also see a kettle, likely bought from the ward budget intended for patients, but used exclusively by the staff.
Considering the Halfway House was managed by two nurses for twenty patients at night (a 1:10 ratio), the staff doubled in the morning to four nurses, plus the Nursing Officer, the Deputy, and a clerk. With an average of five staff members, the patient count actually dropped to about ten, as many went to work or out on leave (this was before COVID-19, after which they locked everyone in). This meant a ratio of one staff member for every two patients (1:2).
If the nurses had so little to do that they slept through the night, they had even less to do in the morning. While they "abusively" slept at night, during the day they ran private errands — going to the beautician, shopping, paying car insurance, or taking their cars for servicing. They could even sleep during the day, as those beds were available to them 24/7, unlike the patients who were restricted to two hours after dinner.
When people say psychiatric staff have a stressful job, rest assured it is only "stressful" because they have so little to do that a shift feels a century long. It becomes clear why they wasted hospital money intended for patients on beds and sofas for themselves.
When I used to work shifts at Enemalta, some of us would occasionally abuse the system and sleep during the night. However, this was always done in secret; we would use our uniforms as pillows and sleep on cardboard on the floor. No one ever dared to bring a full bed and sofa into the staff room — let alone have those beds paid for fraudulently with taxpayer money intended for the Corporation!
This behavior wasn't unique to the Halfway House; it is endemic among the staff of this "fake" hospital. As you can see in the video, when I walked down the corridor past the clinic and looked into the large internal courtyard, almost everywhere was in total darkness — including the FW3A staff room on the other side. The staff abuse their positions so blatantly, right in the faces of the patients they mistreat, without any fear of dismissal. They know that if the corrupt authorities took action against one of them, they would have to dismiss almost everyone. Consequently, the staff dictates the rules rather than following them. (It is much like how the GWU operated under the PN government at Enemalta: the administration ignored the managers — the patients — to please the officials — the staff).
Another massive fraud in this hospital involved the distribution of food. More food was intentionally ordered for patients than necessary so that the staff could help themselves. Originally, staff had the privilege of free food at the mess hall, but during COVID-19, when the mess was converted into a patient ward, the food began being distributed directly to the wards. This resulted in staff taking food home or using it to feed their own animals. Imagine how much more was wasted before COVID, when many patients were out on leave.
Earlier, I mentioned an incident where my medication dosage was vilely doubled because I tried to report the theft of food at MW3A. On that occasion, a nurse threw away food I had set aside. Because only about 25 out of 40 patients were present for meals, I would take an extra plate to feed the cats behind the ward and the two dogs in the MW3A garden. Those dogs were only given the "leftovers of the leftovers" — literally just bones — and they were so hungry they ate them. In an act of revenge, because I was "stealing" from the food the staff wanted to take home for their own animals, they prevented me from feeding the strays by throwing the food away.
To make matters even more vile, after I reported this to the Commissioner for Mental Health, he likely issued a directive through the CEO to prohibit patients from feeding animals. Indirectly, this ensured more food remained for the staff to feast on. It is a sickening irony: I was maliciously framed and labeled a "cat killer," yet it was the Commissioner and the CEO who, without conscience, let the hospital animals go hungry just to please the staff and spite the patients. A patient is left without dignity, abandoned to their fate, while the staff is always excused and supported by the authorities. This is exactly why the situation has degenerated to the point where staff spend nearly the entire night asleep — because the corrupt authorities back their every move.

To return to the massive fraud in food distribution, consider the patients who end up overweight. This happens not only due to the side effects of the drugs and injections used to sedate and destroy them, but also because of the sedentary lifestyle they are forced into — having nothing to do but sit on a sofa all day long.
Now, compare them with some of the staff, who are often even more overweight for the same reason: they have nothing to do while earning a salary. They spend their shifts sleeping and gorging themselves on food intended for the patients, or taking it home to feed their own animals. In fact, employing an gluttonous nurse and putting them in charge of food distribution is like employing a thief as a bank guard and handing him the key to the safe; you would be shocked at the size of their appetite. It isn't hard to guess why some staff end up so large.
In the same way that an overweight staff member or a heavy smoker clearly doesn't care about their own health, you can imagine how little they care about the health of others. With few exceptions, they have no regard for their patients — especially vulnerable patients who have been labeled "mental," stripped of their dignity, and left voiceless. Expect these people to constantly invent new rules to humiliate and abuse patients further, for that is how they treat us: as nothing more than slaves and imbeciles.
As I mentioned previously, the staff abuse their positions — sleeping on duty, stealing patient food, inventing miserable rules, and transferring patients as revenge for reporting them — because they see that those above them, the doctors and psychiatrists, do even worse. This creates a cycle of excuses: the staff simply follow the sadistic examples of their bosses. As the Maltese saying goes: “Għidli ma’ min tagħmilha u ngħidlek x’int” (“Tell me who your friends are, and I’ll tell you who you are”).
I previously wondered how psychiatrists manage to juggle multiple jobs — full-time hospital positions, university lectures, private clinics, and acting as court experts — all while pocketing multiple salaries. I will give you a clue as to how they pull off this fraud, and I will let you draw your own conclusions.
Further up, I listed the eleven clinical firms at Mount Carmel Hospital. In many cases, during ward rounds, the Psychiatrist listed as the head of the firm is nowhere to be found. Instead, a new graduate appears in their place. For almost every patient this graduate sees, they have to phone the consultant — who is likely not at work despite it being their "full-time" shift — to discuss how to drug the patient. The hospital likely even pays for the mobile phone and internet used for these calls. Essentially, the corrupt administration wastes money to allow heads of firms to be absent from their posts.
Later in the day, these consultants might show up for a few hours to discuss which drugs to experiment with next. What is even more vile is that during the few hours they actually spend at their government jobs, they likely use the time to promote their private practices (say: Anton Grech, David Cassar and Hector Cutajar) or perform work for other income sources. They write court reports, prepare university lectures, or rehearse the nonsense they plan to say on TV programs.
This is exactly what David Cassar did when he came to see me to write his "fake" court reports. In my first case (Friday, 21-Jun-2002) and my second (Monday, 2-Jun-2014), he visited me on weekdays during the hours he was supposedly working his full-time hospital job. He was pocketing income from two sources at once — or, as we say of corrupt politicians, “jiekol b'żewġt iħluq” (“eating with two mouths”). The same happens when they lecture at the University for €80 an hour during hospital shifts, or testify in court without taking vacation leave.
So, why blame a nurse for running errands during the day or sleeping through a night shift? They see their superiors setting the example of blatant corruption. Everyone — psychiatrists and staff alike — perseveres in these abuses because they know no one can take action against them without exposing their own guilt. As the saying goes, “a rotten apple spoils the barrel.”
They work hand-in-hand to destroy patients' health with pills and injections, leaving them too sedated and "imbecilic" to report these blatant abuses. They cover for each other and scratch each other's backs. God forbid a patient tries to reveal the fraud of one, let alone both; they will unite like a Masonic lodge to make that person's life a living hell, silencing them with "chemical restraints" or a total "restriction of communication."
 The photo above captures nurses celebrating "Happy Nurses Day 2020" outside the ward, while patients remained locked inside — as they had been since March 12, 2020, due to COVID-19.
The photo above captures nurses celebrating "Happy Nurses Day 2020" outside the ward, while patients remained locked inside — as they had been since March 12, 2020, due to COVID-19.
Second from the right is Glenn Galea. Second from the left is the nurse who worked shifts with him, who habitually locked female patients away for half an hour (visible in the video above). As the saying goes, "birds of a feather flock together."
In his Facebook post, Galea complained, "It is not what I envisioned." Presumably, because of the lockdown, he found himself doing more work than his usual "nothing," and had fewer opportunities to take home patients' food. Regarding the rest of the group, refer back to the previous paragraph: with an average of five staff members on duty, they mostly had nothing to do.
If anyone thought the previous video of that nurse sleeping was a one-off event, this video proves otherwise. Here he is again, being paid to sleep an entire night. This time, he slept from 10:00 PM until 5:00 AM — two hours longer than before — as if that makes any difference to the corrupt hospital authorities.
In these videos, another female nurse was on overtime instead of the one who worked shifts with him. She pocketed 1.5 times her normal pay just to spend the night sleeping. Why should Melvin Theuma be blamed for being paid for three months of work he never did, or why should I be blamed for the "crucifixion" of animals already found dead, rather than those who killed them with their cars or the hunters who kill birds for sport? Truly, "Why do you see the speck in your brother's eye and pay no attention to the log in your own eye?" (Matthew 7:3).
This is yet another video of the "dedicated" Glenn Galea being paid to sleep. Consider this: if a child reports a teacher’s abuse at school, that teacher is often suspended immediately pending investigation. In a mental institution, the opposite happens. They take revenge on the patient for daring to report staff abuse — as happened to me — while the staff are excused for their corrupt practices.
If you are still in doubt, here is another video of Galea sleeping. His shift repeatef every five days. Contrast this with a new graduate in the private sector, where employers exploit them for unpaid extra hours under the guise of "being professional."
This video is from another shift where the nurse slept with the lights on for over four hours straight. I didn't film the remaining two hours under the assumption that he was entitled to a two-hour break. However, he was at least not as sadistic as that pathetic nurse Glenn Galea, who locked the male toilets. Note again that the clinic remained closed all night; the staff simply do not care if the telephone rings. They are completely devoid of ethics or decency.
The Cost of Truth: How Reporting Abuse Lost Me My Freedom
Around May 2020, I was fighting on behalf of the patients, demanding that the Hospital Authorities distribute dessert as they had in years past. To support my argument, I sent the first video in this series showing Glenn Galea sleeping through his shift. I argued that if there is money to pay him for doing nothing but sleeping, there should be money for a €1 dessert for patients.
But as I mentioned, the sadistic staff and psychiatrists at Mount Carmel Hospital cover for one another. What happened next was incredible: just three days after I emailed the newly appointed CEO, Stephanie Xuereb, and Customer Care — which falls under Psychiatrist Anton Grech — retaliation followed. On June 12, 2020 (the 18th anniversary of my abusive 2002 confinement by Psychiatrist David Cassar and Magistrate Carol Peralta), I was transferred and locked in Male Ward 1.
In that ward, I was surrounded by primitive conditions and patients with poor hygiene. I was stripped of my phone and laptop, forced to sit all day on a sofa inhaling second-hand smoke. I was placed on "Level 1" 24/7 supervision, and they issued a "Restriction of Freedom of Communication Order" (see image below) to silence me. They wanted to break my spirit so they could justify drugging me into a stupor. If my sister hadn't stepped in and emailed Commissioner John Cachia (link), Psychiatrist David Cassar (link) and the police (link 1, link 2), they would have succeeded. It makes it easy to understand what happened to Mangion and Harrington at the Forensic Ward; when you are left alone, they can silence you permanently.
"Break the Silence": The Hypocrisy of Malta’s Mental Health Authorities
 Above is the "Restriction of Freedom of Communication Order" issued by the Office of the Commissioner for Mental Health, John Cachia, on behalf of Psychiatrist David Cassar The Commissioner did not even have the decency to hear my version of events before signing it (refer to the emails sent by my sister). He so much considered patients as "scum," that for him it was a waste of time to listen to us, let alone protect us from abuse. Significantly, the order contained no expiration date — a tactic clearly designed to instill despair.
Above is the "Restriction of Freedom of Communication Order" issued by the Office of the Commissioner for Mental Health, John Cachia, on behalf of Psychiatrist David Cassar The Commissioner did not even have the decency to hear my version of events before signing it (refer to the emails sent by my sister). He so much considered patients as "scum," that for him it was a waste of time to listen to us, let alone protect us from abuse. Significantly, the order contained no expiration date — a tactic clearly designed to instill despair.
With a simple stroke of a pen and the usual blatant lies, they can render you voiceless and destroy you with injections. Even the corrupt police saw nothing wrong with this (link 1, link 2), leaving me entirely in the hands of psychiatrists to do as they pleased. It is like a child in an orphanage pleading for help, only to be abandoned to his fate.
Meanwhile, these same people hold press conferences with slogans like “BREAK THE SILENCE – We cannot continue to let patients and families suffer alone.” The hypocrisy is staggering. In public, they preach compassion; behind closed doors, they officially approve your silencing.
Naturally, no action was ever taken against that pathetic nurse. He still works at the hospital, still sleeps through the night, still steals the patients' food, and still locks the toilets so that a flushing sound won't wake him. But for me — the whistleblower — the revenge was swift and severe. My communication was restricted until July 18, 2020, and I was locked in Ward 1 without a laptop or phone for 43 days.
It is frightening to remember how they intended to ruin my health and disable me with psychiatric medication. Without my sister’s help, they might have succeeded. Because I remained calm despite the trauma of Ward 1, they couldn't find an excuse to overdose me. They claimed my mental health had "deteriorated" because I reported staff abuse, yet my emails — which I have uploaded here — prove I was far from "crazy". Psychiatrists are blatant liars and manipulators of facts.
If that weren’t enough, on August 12, 2020 — within two months of being sent to Ward 1 — the staff at Half Way House sought further revenge. They falsely accused me of saying I wanted to stab Psychiatrist David Cassar with a knife. I have no history of violence; had this been true, the police would have been called to interrogate me and search for a weapon. Instead, using this blatant lie as an excuse, they transferred me to Male Ward 7. My medication was increased by 50% (from 10mg to 15mg of Olanzapine daily), I was placed under 24/7 Level 1 supervision, and a new communication restriction was issued.
This happened immediately after I reported another staff member for sleeping through the night. Rather than transferring the negligent staff, the CEO had me transferred. During this move, a staff intentionally broke my laptop. I was forced to cover the €1,000 repair and data recovery costs myself; two years later, they only refunded me a measly €140 for the screen.
You must be incredibly mentally strong to survive such sadism and injustice. By late August 2020, they even cut the free Wi-Fi in Ward 7 to further isolate and silence me. They had planned to prohibit smartphones post-COVID so that patients cannot gather evidence of abuse. Without proof, a patient’s report is easily labeled an "inappropriate belief," providing an excuse to drug them into silence.
A Stolen Goodbye: How Psychiatry Kept Me from My Dying Mother
Then came a third communication restriction order within a year, issued on June 24, 2021, by Psychiatrist Catherine Dimech. This was particularly cruel, as I had recently begged her to let me visit my elderly mother, who was dying. She passed away that September without me being able to see her one last time. The order was issued on the pretext that I was refusing my medication — even though the previous psychiatrist, Joe Vella Baldacchino, had allowed it, and despite my rights under Article 3.1.i of the Mental Health Act, (see that Consent Form).
The Sleeping Guards of Mount Carmel: Corruption and Collusion
 Being placed on "Level 1" observation means having a staff member watching you at all times (a 1:1 ratio). It is deeply humiliating to be followed everywhere, even to the toilet. The document above is from my hospital file during my 2014 confinement at the Forensic Ward (under Psychiatrist Hector Cutajar, on behalf of Maria Axiak). I was subjected to this same "Level 1" treatment in Wards 1 and 7 in 2020 as retaliation for reporting staff abuse.
Being placed on "Level 1" observation means having a staff member watching you at all times (a 1:1 ratio). It is deeply humiliating to be followed everywhere, even to the toilet. The document above is from my hospital file during my 2014 confinement at the Forensic Ward (under Psychiatrist Hector Cutajar, on behalf of Maria Axiak). I was subjected to this same "Level 1" treatment in Wards 1 and 7 in 2020 as retaliation for reporting staff abuse.
The staff assigned to watch me — often foreign workers — literally had nothing to do. They were paid to simply sit and follow me. They would spend their shifts chatting on their phones and browsing the internet. In any other workplace, an employee caught on Facebook all day would be warned or dismissed. But here, it is treated as normal. They enjoy 24/7 free Wi-Fi while the patients, whom the Wi-Fi was intended for, are restricted.
According to Article 3.1.r of the Mental Health Act, patients should have "free and unrestricted communication with the outside world." Yet, in Ward 1, patients were only allowed 30 minutes of internet access on Sundays via a shared laptop. While staff used the Wi-Fi 100% of the time, patients were restricted to just 0.29% of the week. They treat patients as scum, worse than animals, while profiting at our expense.
When I was briefly returned to the Halfway House before being shuffled like a "sack of potatoes" to Ward 7, they put me on Level 2. The reason? A nurse reported me for the "sin" of feeding cats and helping other patients wash dishes. This was clearly revenge for my report on Glenn Galea. This nurse, who also steals patient food to feed her own dogs, knew she would never face consequences. The corrupt authorities and sadistic psychiatrists use these trivial reports as an excuse to "experiment" on patients with even more potent drugs, ensuring the staff can continue to sleep and steal in peace.
My first Treatment Order
 Above is an extract from my hospital file regarding a Treatment Order issued by Psychiatrist David Cassar on June 25, 2002, when I was transferred from Male Ward 10 to the Mixed Admission Ward. Note the identical wording and handwriting, which clearly belong to Dr. Cassar, despite the use of a different pen — as if to create the illusion that two psychiatrists arrived at this conclusion independently. On the right-hand page, Psychiatrist Hector Cutajar acts as a mere rubber stamp. As we say in Maltese, "Kappell ma jmerix lill-ieħor" (One official does not contradict another). I even suspect that the signature might not be Cutajar’s at all, but rather signed on his behalf by Cassar.
Above is an extract from my hospital file regarding a Treatment Order issued by Psychiatrist David Cassar on June 25, 2002, when I was transferred from Male Ward 10 to the Mixed Admission Ward. Note the identical wording and handwriting, which clearly belong to Dr. Cassar, despite the use of a different pen — as if to create the illusion that two psychiatrists arrived at this conclusion independently. On the right-hand page, Psychiatrist Hector Cutajar acts as a mere rubber stamp. As we say in Maltese, "Kappell ma jmerix lill-ieħor" (One official does not contradict another). I even suspect that the signature might not be Cutajar’s at all, but rather signed on his behalf by Cassar.
They claimed I was suffering from "paranoid psychosis" and had "no insight," yet they provided no scientific evidence to support this diagnosis. I was locked up for "non-compliance," but the real goal was to silence me. They didn't want me reporting how Magistrate Carol Peralta threatened to smash me against a wall in open court. These psychiatrists don't provide "treatment" for health; they use it as a tool for ulterior motives to protect the powerful and crush their victims.
Get Busy Living or Get Busy Dying: My Years in the Cage
The video above shows an old ward similar to Male Ward 10, where I was held in 2002. The layout consisted of a row of cells with a corridor on one side; once they locked the door, they supervised you through a window from the opposite corridor. During the sweltering summer of 2002 — while the World Cup was taking place in Japan and South Korea — we were locked in those rooms for 21 hours a day. Usually, we had only a mattress on the floor and a toilet in the corner.
We were permitted to speak to relatives through Perspex for only 15 minutes, with one five-minute phone call per day. This environment is exactly what you need to make someone’s mental health deteriorate, yet I remained calm — even during the first ten days before they began drugging me by force, and despite the knowledge that Psychiatrist David Cassar had nearly caused me to lose my full-time job.
In my teens, I remember watching the film Le Ali della Libertà (The Shawshank Redemption). I never imagined I would end up living that story myself. Certain quotes from that film have remained etched in my mind for years; hearing them again makes my blood run cold, as I have lived them through the "fake" branch of medicine known as Psychiatry:
- "Feel bad about it if you want, but you didn’t pull the trigger."
- "No, I didn't. Somebody else did. And I wound up in here."
- "Bad luck, I guess. It floats around. It's got to land on somebody. It was my turn, that's all."
- "I just didn't expect the storm would last as long as it has."
- "I guess it comes down to a simple choice, really: Get busy living, or get busy dying."
Fortunately, the fight against psychiatry is a global one. Countless lawsuits have already been won against big pharmaceutical brands (see the Risperdal and Zyprexa settlements) and for psychiatric malpractice. Global platforms like Mad In America, the Citizens Commission on Human Rights and the Center for the Human Rights of Users and Survivors of Psychiatry now stand up for survivors. Sites like KnowYourDrugs also provide essential information on the real dangers and side effects of psychiatric drugs.

The Sabotaged Life: How Psychiatry Turned a Victim into a Patient
Around June or July 2020, while I was locked in Ward 1, I met a patient named JX This is his story.
Having lost his mother at the age of eight, JX spent four years living in an orphanage. Despite these hardships, he completed secondary school and dreamed of further study. However, his father — a heavy smoker — pressured him to work instead, refusing to pay for exam fees or allow him pocket money for friends. Driven to a breaking point by this lack of support, the 20-year-old JX took out his frustration on a statue of Our Lady, smashing it at the local police station. He was locked in Mount Carmel Hospital (MCH) for three weeks. The system blamed him — not his father’s neglect or the obstacles placed in his career path.
JX eventually found a job and returned to school, but the pestering continued. His father would even switch off the computer during school assignments to "save" on electricity. When he could stand it no longer, JX broke the refrigerator and was sent back to MCH. Though initially prescribed Paxetine and Risperdal, he stopped taking them because they caused extreme fatigue and sexual dysfunction. When Psychiatrist David Cassar confronted him, JX claimed he had only "missed a few doses" to avoid being forced onto an injection. The lie backfired: Cassar put him on Fluanxol injections. The side effects were devastating — stiffness and restlessness so severe that he could no longer play football.
The stigma followed him. A girlfriend broke up with him, likely fearing his diagnosis and the effects of the medication on future children. When he tried to reconcile at her doorstep, he was locked up again. Under Cassar’s care, he was given Valium, which caused delirium, leading back to higher doses of Fluanxol and other pills.
Remarkably, JX still managed to graduate from MCAST. However, the friction with his father — aggravated by two years of psychiatric drugs — eventually led to a physical fight that made the local news. Because of his "mental patient" label, JX was blamed while his father was excused. Cassar switched him to Risperdal injections, which again caused sterility, forcing him to give up on romantic relationships.
After four years of this cycle, JX refused his injection out of sheer frustration. The police arrived at his door, and he was locked in MCH for three weeks under a new Treatment Order. This is where I met him. They claimed he had threatened to "contact a bomb dealer" unless the order was removed. Again, common sense suggests that if this were a real threat, the police would have interrogated him and investigated the dealer. Instead, the hospital simply used it as an excuse to destroy him further with Lithium and high-dose Risperdal (75mg–100mg fortnightly).
Psychiatry didn't save JX; it dismantled him. At just 29 years old, he had been rendered "fat," physically stiff, and perpetually exhausted by a cocktail of heavy medication. He was on the verge of losing his job, which would have stripped him of his final shred of freedom and delivered him right back into the hands of his father or the hospital wards. The system had stolen his ability to enjoy life to the point that suicide felt like his only escape. This was the grim reality of the psychiatric machine: it doesn't heal you; it ensures you always lose.
The Lifelong Sentence: How One Diagnosis Destroyed a Future

Another patient, RZ, suffered frequent physical abuse at the hands of his father, who would beat and sometimes even bite him. Following the death of RZ's mother, his father moved a new partner into the family home. When RZ voiced his opposition, his father threatened to throw him onto the streets — penniless and starving — rather than ask his partner to leave.
This domestic tension culminated in yet another fight. Despite being the victimized teenager in the situation, RZ was blamed for the conflict. He soon became the latest victim of Psychiatrist David Cassar at Mount Carmel Hospital. Initially, Cassar prescribed large pills; when RZ struggled to swallow them, the doctor offered a "choice" to secure his release: a bi-weekly injection of Clopixol. RZ, young and unsuspicious, accepted the treatment, believing it would only last a few months.
The side effects of Clopixol were devastating. RZ suffered from severe eczema, dermatitis, and purpura—bleeding under the skin that manifested as painful red and purple discolorations. Frustrated and ashamed, he began to isolate himself. He feared his friends would think he had a contagious disease and stopped swimming or wearing short-sleeved clothes to hide the marks.
Years passed, and his father eventually died. Later, a dispute with a neighbor over late-night construction led to a confrontation involving the police. In court, two psychiatrists simply built upon the original narrative established years prior by David Cassar. They labeled RZ as "unable to control his anger" — an irony, given that his frustration likely stemmed from the very drugs and systemic abuse that had ruined his youth.
Using this as an excuse to further medicate him, the court sentenced him to two years in the forensic section of Mount Carmel. When his release date finally arrived, social workers deemed his home uninhabitable due to a lack of electricity. Rather than providing support, the psychiatrists kept him locked away in a different section of the hospital.
This is where I met him: another life turned into a living hell, systematically ruined by the cruelty of the psychiatric system.
Pills on an Empty Stomach: A Case of Institutional Indifference
KG is a patient who was sentenced to Mount Carmel Hospital following a court case. For years, he was prescribed injections at such high dosages that he often struggled simply to walk. As he aged, the injections were discontinued, but they were replaced by an even larger regimen of oral pills.
Among the many side effects of this "poison" is severe gastrointestinal distress. He suffers from chronic constipation for days at a time, followed by bouts of painful diarrhea. When he finally complained to the nurses about his suffering, they called in a hospital doctor. The solution offered was a three-day fast — drinking only water and eating no food — in preparation for medical tests at Mater Dei Hospital.
What I found truly frightening was watching him forced to swallow a handful of pills — the very source of his ailments — day after day on a completely empty stomach. This blatant disregard for his physical well-being seemed to be of no concern at all to the nurses or the staff. It was a harrowing display of institutional indifference.
The Parkinsonian "Cure"
In 2022, I met LS, a man living with severe autism whose frustration occasionally led him to punch himself in the forehead. To "treat" this, he was prescribed the diabolic injection Risperdal Consta. This "poison" possibly resulted in him suffering from Parkinsonism and other debilitating side effects. In the twisted mentality of modern psychiatry, a slow and premature death via medication is considered less harmful than an occasional, non-life-threatening punch to the forehead — though, predictably, the injection did nothing to alleviate his self-harm.
When I raised my concerns with a staff member, I was cut short with the words: "Għax hekk għandu bżonn" (Because that is what he needs).
You will not find these stories in our fake local media. To stay in business, their sponsors dictate what is written and what is suppressed. Expect nothing but eulogies to psychiatry, designed to trap and exploit the next victim in an insatiable greed for profit. They claim that "independent journalism costs money," but in Malta, true independence makes enemies and can cost you your life. It is the biased journalism, the kind that ignores the suffering of people like LS, that makes the easy money.
The Contradictions of Psychiatric Logic: Guinea Pigs of the State
 Psychiatrist Rachel Taylor East
Psychiatrist Rachel Taylor East Psychiatrist Nigel Camilleri
Psychiatrist Nigel Camilleri Psychiatrist Kristian Sant mal-kelb
Psychiatrist Kristian Sant mal-kelbTo further illustrate that psychiatry has been since ever a system riddled with internal contradictions, I need only point to my own history. For years, I successfully managed a high-responsibility full-time job, overseeing a team that trusted my leadership. I lived what any observer would call a "normal" life; no one in my professional or social circles ever suspected me of being anything other than high-functioning and stable.
The "Symptom" Paradox: In response to what was essentially my provocative prank involving animal crucifixions, psychiatry reached for its usual bag of 'fake labels' — diagnosing me with Schizotypal Personality Disorder and inventing convenient 'instances of mental alteration' to explain away my otherwise stable life. According to their nonsensical logic, my "symptoms" were not a constant state of being, but rather something that manifested only in highly specific, ritualistic windows:
— The moments I stopped while cycling to collect a feline carcass.
— The process of cleaning and freezing it.
— The monthly ritual — usually on the 16th — of thawing, crucifying, and displaying the remains in my hometown.
The absurdity lies in the claim that a person can be perfectly rational for 29 days of the month, only to be "disordered" during the specific hours of a chosen ritual.
Precedent: The "Convenient" Psychosis:This selective labeling is a recurring theme. Years ago, a young man dubbed the "Teen Bomber" was subjected to a 13-page report by psychiatrists Rachel Taylor East, Nigel Camilleri, and Kristian Sant. They concluded he suffered from "substance-induced psychosis" — a state of insanity that supposedly existed only at the precise moments he was manufacturing and placing explosives.
This mirrors the testimony of Park Dietz in the Jeffrey Dahmer case. Dietz argued that Dahmer drank alcohol to "overcome inhibition," suggesting that without the substance, his "true" state was one of being inhibited against killing.
The Logical Loophole: If a substance is required to "overcome inhibition," what prompted the initial decision to consume the substance? Is there a fabricated disorder for the intent that precedes the "psychosis"?
The Systemic Trap: In reality, individuals like this young man — and myself — are treated as little more than guinea pigs for a system eager to experiment with the "venom" of psychiatric medication. For what should have been viewed as a youthful stint of rebellion meriting a mere suspended sentence, he is now caught in a lifelong cycle of institutionalization. Having already endured months of detention at Mount Carmel Hospital, his future and career are being dismantled before they have even truly begun.
The Ultimate Irony: The irony of the Maltese psychiatric and legal system is staggering when viewed against the country's political history. In the 1980s, the two main political parties engaged in a literal campaign of terror that "was not simply hallmarked by the bomb attacks." The Labour government went so far as to oversee the death of an opposition supporter, frame the innocent, and participate in police beatings that ended with a man being killed and dumped under a bridge.
Yet, when the state commits these acts, it is "politics." When an individual acts outside of social norms, it is a "disorder" requiring a lifetime of chemical intervention.
Double Standards: Why Some Deaths Merit Inquiries and Others Are Ignored
The history of Mount Carmel is littered with tragic, preventable deaths. Take the case of SC, a patient I knew in Male Ward 7. He was transferred to "Dar Victoria" in Marsa, where, around April 22, 2022, he choked to death. The staff, likely as incompetent as those in the hospital, failed to save him. As is typical with fatalities involving psychiatric patients, there was no public outcry or investigation.
Contrast this with the case of Stephen Mangion, where a magisterial inquiry was immediately launched to investigate potential shortcomings at Mater Dei’s Emergency Department. Why the double standard?
When I was locked in Male Ward 3A years ago, a patient named JG choked in the hospital canteen and died because staff failed to intervene. Later, in Male Ward 7, I personally witnessed two frightening scenes. On July 25, 2021, a patient, SLV, choked on rabbit meat. He was only saved because nurses from Mater Dei happened to be nearby and rushed in to assist.
However, MA was not so lucky on November 15, 2020. He choked on a piece of bread — something that should have softened with saliva. His inability to swallow was likely a direct side effect of the Risperdal injection he had been prescribed: Risperidone-Induced Tardive Pharyngeal Dystonia (see also: drug-induced dysphagia). When he began to choke, a psychiatrist — thinking he knew better than anyone else — took charge. Kulħadd warrablu (everyone gave way to him), and the result was a fatality. As one might expect from a psychiatrist playing at emergency medicine, he didn't save the life; he sent the man to his maker.
Tragically, SLV’s luck eventually ran out. On February 11, 2024, he choked again in a different ward at Mount Carmel. This time, there were no Mater Dei staff nearby to rescue him — only the Mount Carmel nurses who, as was reportedly their custom, entered their night shifts prepared for sleep rather than vigilance. Predictably, the incident was fatal.
Silent Witnesses and Static Authorities: The Tragedy of Avoidable Fatalities — the Devaluation of Life at Mount Carmel Hospital

Equipped for everything, prepared for nothing. Male Ward 7’s emergency trolley features full intubation kits and LifeVac devices, supported by hospital-wide AEDs (Automated Emergency Defibrillator - analyzes the heart's rhythm and, if necessary, delivers an electrical shock, or defibrillation, to help the heart re-establish an effective rhythm). Sadly, high-tech hardware cannot compensate for a lack of clinical competence..
With the sole exception of patient SC, the fatalities mentioned above did not occur in the homes of inexperienced relatives who might lack the knowledge to handle such emergencies. Instead, they took place within a hospital — an environment supposedly staffed by professionals competent in emergency response. Even more galling is the fact that these deaths occurred within wards equipped with emergency trolleys (see image above) specifically designed for these crises.
The fundamental clinical priority should have been the immediate removal of the airway blockage. To do otherwise is as nonsensical as performing CPR on an accident victim without first stopping their arterial bleeding. In the specific case of patient MA, the rigid hierarchy of the ward proved fatal; no nurse dared to direct the Psychiatrist. It is highly likely that a senior consultant was unwilling to "soil" his hands to clear a patient’s airway, and the subsequent actions taken likely served only to further obstruct the passage.
Despite these clear failures, the hospital administration and relevant authorities have never initiated a formal investigation. They have consistently refused to interview witnesses or address the documented shortcomings sent to them (as seen in these communications to the Commissioner for Mental Health (link), the Director (Human Rights) (link), and the Commissioners for Health within the Ombudsman's Office (link1, link2).
It further reveals a grim reality at Mount Carmel Hospital: patients are stripped of their dignity, treated worse than animals, and viewed as mere "guinea pigs" or statistics. To the administration, a death is not a tragedy—it is simply one less patient to manage, and another bed cleared for the next victim. The following email excerpts further highlight the total impunity enjoyed by a staff whose incompetence and sadistic abuses are perpetually shielded from accountability.
Excuse my late reply, as I was busy fighting my case on other fronts while concurrently trying to help other victims. Of course, I also do not have the luxury of a laptop at my disposal, for the one I had was smashed by staff for reporting their abuses, and I have been prohibited from using one again; so, only an old smartphone has to save my day.
First, I wanted to clarify a small, likely unintentional mistake in your first paragraph, which should have read "2 years before" (not a year before), referring to that tragic incident of 15-Nov-20.
What is unbelievable is that despite the fact that I, a mere patient, had played my part as a first-hand eyewitness and had written to the relevant authorities — including your predecessor — months before I wrote to you, no one ever bothered to investigate. Let alone did they take any serious actions to prevent such incidents from happening again; they just vilely brushed it under the carpet. This confirms further how, for them, a patient is a nullity whose calls are simply ignored — just an unwanted nuisance not to waste time on, regardless of the severity of the complaints.
This is done not only to discourage a patient from having the audacity to report again, knowing his cries will always fall on deaf ears, but even worse, to intimidate him. He is made to suffer repercussions himself for daring to uncover abuses, paying with his own health by being poisoned further with drugs, and being silenced and made voiceless by being locked in wards with less freedom. Even his most sentimental possessions are vandalized, as they did with my laptop and the multitude of data I had accumulated in it.
The staff are treated as demi-gods in contrast to a patient's life, which is so worthless and meaningless to them that, whatever the shortcomings, incompetence, and wrongdoings of the staff at the expense of their miserable patients, they are always excused and covered up. Such was the case with Psychiatrist Hector Cutajar, who not only wasn't sacked — let alone brought for questioning before a board or prosecuted — but even ended up promoted anyway and is still ruining patients' lives with his sadism.
Now that I have written to you presenting facts and arguments, I was hoping I would be given the chance to at least testify further regarding the incompetent nurses present on that tragic day. However, as I had perfectly predicted, you opted to let these "big heads" and "friends of friends" get away with it, just as the corrupt others had done before you. As has always been the custom in corrupt Malta, those "characteristics" place them above the law, privileged to enjoy a culture of complete impunity, while the patients are just their umpteenth victims who have to pay the ultimate price for all this.
Imagine taking your beloved cat to a vet and paying him good money, only for him — through his incompetence — to give it back to you dead, when others would have easily saved it and returned it to you completely healthy to enjoy each other's company for many more years. Would you remain silent and let him get away with it that easily?
Now, this wasn't a mere pet, but a human being who ended up, like me, kidnapped unjustly in this hospital to be abused and experimented upon at leisure with the poison of psychiatric medication and its terrible side effects. It is actually a million times worse than the treatment of animals; by today's standards, I presume research on animals that produces such devastating effects — like making one sick with drug-induced parkinsonism — has long been prohibited. The only thing animals and patients in this hospital still have in common is that both are completely voiceless.
That tragic death — which you called "regretful" and I call "shameful" — as well as others, would have been avoided had the authorities taken action when, in the past and just months before that incident, I had reported other staff abuses in vain.
Instead of taking the opportunity to implement reforms that would make staff concentrate on their work and enforce discipline and a sense of duty, the authorities kept covering up their corrupt practices. They did this by transferring someone like me — who was watching them — to other wards, leaving the doors wide open for them to persevere in their malpractices unhindered. This was done to intimidate and further abuse me as a lesson to others; it was an indirect show of solidarity and support from the authorities for the staff's malpractices, regardless of their severity.
They never dare to investigate if it means incriminating staff or putting them in a bad light. For them, the most "sadistic wrongdoing" is a mere miserable patient having the audacity to speak. This capacity to report must be prevented at all costs by destroying the patient psychologically — keeping him always locked away without any permissions, not even for a little fresh air, even if it means blatant violations of the UN Charter of basic human rights.
By drugging and incapacitating a patient, they deny him the capability of ever daring to report again. It serves as a lesson to others that they will suffer the most sadistic consequences if they try. This further instills a climate of terror to make voiceless patients even more voiceless, stigmatizing them through the lies and sadistic labels of Psychiatry, as happened with me, to shut their mouths before they even have the chance to open them (dismissing it as just their "delusion of persecution").
How can patients' lives not be at stake when malpractices of all sorts imaginable occur and the authorities do nothing to stop them — even when they are made fully aware of them? To mention just a few from the multitude I have reported: staff eat food intended for patients and take it home to feed themselves, their families, and their animals (as a sort of "extra salary"). The first time I reported this, I was prohibited from using the meat in my own meal to feed the cats, just so more would remain for the staff to take home. They take the Ecopure water for themselves, while for the patients, they continue making coffee and squash out of tap water.
They spend entire nights sleeping on new sheets, which they then reuse to make patients' beds the following morning. They spend their days playing on computers using government-paid internet, wasting bandwidth on everything except work-related matters (save for the occasional email). When it is time for a shift change, the bulk of them leave about an hour early, leaving the ward attended by only two staff members. The punch clocks are only for those employed by Healthmark; literally, the government is paying the salary of a doctor to receive the service of a carer or a cleaner.
Our ward head has even abusively dedicated a room intended as an office within the ward — equipped with a government computer and internet — to serve instead as childcare for her nephew. She brought him to spend the entire summer playing inside, while patients like me were treated like lepers, forced to have visits from behind perspex because of COVID-19 measures. Meanwhile, we cannot even use the ward laptop intended for patients' use (which is rarely used, perhaps only to communicate with a social worker).
The ward head often arrives an hour late but records it as if she arrived on time. Yet, patients who go out on leave must do so within strictly limited times. The staff set the worst possible example in everything, but expect patients to follow every rule they invent for even the slightest mishap. They run private errands when they are supposed to be at their workplace and take breaks twice as long as they are entitled to, in staff rooms equipped with beds, pillows, and lockers.
They are always believed when they lie and frame patients who dare to report them, paving the way for sadistic Psychiatrists to do the rest — drugging them and experimenting on them further. They are always excused when they abuse patients and are even assisted in their revenge. This includes verbal threats ("Issa jgħidulna min irrapporta, npattuhielu" / "Mur oqgħod ikteb irrapporta, x'min għalik se taħxina?") and locking patients in wards with less freedom. They even destroy belongings to further silence patients, issuing "restriction of freedom of communication" orders lasting one month each to intimidate them. They have even abusively smashed open lockers when patients was out of sight — for example, while locked away because they had tested positive for COVID-19.
What professionalism do you expect from such individuals? Persons without morals or conscience, who come to work to earn a salary while doing nothing, simply accumulating energy for the tasks they have back home or at another job. They do this with the peace of mind that they will never be investigated or held accountable for their malpractices, abuses, wrongdoings, or incompetence — even in the case of an incident that ended in a fatality. The most they ever receive is a fake warning not to repeat the wrongdoing; they are so convinced this is just a formality that, within a few weeks, you see them starting their wrongdoings afresh with even more intensity.
The uncontrolled use of government-provided internet serves only to further distract them from their duties. Senior staff, such as nurses, are even given personal tablets or laptops as part of their employment package, which only serves to make them more incompetent and unprofessional. Rest assured, they use these devices for everything except research on matters concerning their profession.
For all this corruption, it is always the patient who has to pay the greatest price. They pay with their belongings, which are destroyed to the satisfaction of the culprits; they pay with their health, ruined by being drugged further at leisure; and they pay even with their lives due to an incompetence so profound that even a person on the street with basic first-aid knowledge and limited resources would have saved them.
By not taking action against Psychiatrist, Hector Cutajar — letting him go that easily as if nothing happened — you are further reinforcing the precedent already established by those to whom I had reported before. You are signaling that no matter what death or casualty occurs due to staff incompetence, or whatever blatant abuses staff inflict on patients, no action will be taken. It would now appear as blatant discrimination to take action against a nurse or a "man in the street" when no action was taken against this Psychiatrist, who was a million times more incompetent despite being supposedly qualified and holding a more authoritative role.
You are thus intentionally nurturing a climate of complete impunity, where staff have no fear of repercussions regardless of their shortcomings or wrongdoings. This encourages them to persevere in their corrupt practices, knowing well they will never be held accountable. It consolidates the mentality that a patient's life is so worthless that no one gives a damn for its loss. Furthermore, it nurtures a climate of terror for patients; they know their lives are at stake in the hands of these impunity-blessed incompetents, and they fear the sadistic repercussions of simply daring to speak.
The staff find satisfaction in taking their umpteenth revenge on voiceless patients with total liberty. Patients are drugged, poisoned, and sedated further after being maliciously labeled with "inappropriate to inappropriate beliefs," or accused of being "paranoid and suspicious" toward staff, or suffering from "mental confusion." For those who are not easy to manipulate or silence, they even invent the most absurd lies — claiming the patient intended to stab the Psychiatrist or was poisoning cats.
They depict a fighter for rights as a "loser" who wants to commit suicide, using it as an excuse to drug him further, humiliate him, and put him on "Level 1" constant watch with no privacy, as they did with me. Once they intentionally and maliciously label you as "mental," the road is wide open for them to invent the most blatant lies, and everything is easily believed. No one questions them — especially not the sadistic Psychiatrists who seem to be in a competition to see who can outdo the other in their abuses of voiceless, vulnerable patients. You know well that it was not simply
1) the incompetence of the staff that caused that tragic fatality, but even more
2) the climate of terror they instill in patients who dare to report abuses and the subsequent sadistic repercussions they suffer as revenge; and above all,
3) the complete impunity enjoyed by the staff, who know well they are blessed never to be held accountable.
No authority will stand up to them. Even in this case, writing to you as the new Commissioner for "Health" within the Ombudsman’s Office proved once again futile (one wonders if the word "Health" refers to something completely different than its supposed meaning?).
I am attaching two "restriction of freedom of communication" orders I received within the space of two months (1 and
2), issued just months before that tragic incident of 15-Nov-20. These were part of a series of systematic revenges I was forced to pay for reporting abuses. Upon the termination of the second order on 14-Sep-20, they returned my laptop smashed. Even in this case, the CEO chose once again to vilely cover for them, claiming the damage did not result from the negligence or wrongdoings of staff.
However, about a year and a half later, your predecessor exposed her as a liar by mentioning they had given me €140 for the damages (see the emails I forwarded when I first wrote to you). This was out of the €1,000 cost I incurred to repair my laptop and recover my data — and I still do not know if the recovery was completely successful, as they haven't even given me the chance to try it out or use it again. This is a direct example of the culture of complete impunity the staff enjoy, supported by the authorities as mentioned in those three points above, which ultimately led to that tragic fatality.
In one of my first emails to the CEO, I asked her to enforce time-logging to track how the staff are spending — or rather, wasting — their time. Such a move would have proven how over-staffed the hospital is. For example, my ward's capacity was reduced from 28 patients to 21, yet the staff complement was increased around June '21. It also has three Nursing Officers (NOs) plus a secretary blessed with a "cosy" job on the eve of the last election. The hospital could function with just a third of the current staff; the taxpayers' money saved could be diverted toward measures that actually benefit the patients. Instead, the authorities prefer the status quo, as the staff have unions and "friends" to back them and cover for them. In contrast, the miserable patients have no one and even end up being framed. It is a case of being weak with the strong and strong with the weak. Consequently, they would rather keep wasting money on corrupt practices than ever try to tackle them, rewarding the corrupt while playing the miser when it comes to patients' needs — even if it means denying them the absolute basics.
As for the training provided to nursing aides and carers, I learned about its "impact" from the nursing aides themselves; I heard them laughing, saying it would simply serve as an opportunity to earn overtime ("aħjar għax nikluhielu overtime talli noqdu nisimgħu l-ħmerijiet"). That is how "seriously" they took the training, knowing well they would never be held accountable, as has always been the custom.
Regarding the training of doctors and nurses: aren't they supposed to be already qualified in matters of first aid — the basics of the basics? What on earth did they study during their university courses? Can they not conduct research themselves using the government-paid internet provided, rather than being left to use it for trivialities? Are the hospital authorities recruiting incompetents only to have to teach them everything from scratch, again and again, at the taxpayers' expense?
This money could instead be invested in the patients:
— To provide desserts to make up for the often disgusting meals they are fed, or to improve the quality of those meals.
— To offer computer courses or provide free Wi-Fi to patients (currently, the ward TV and internet modem are protected by passwords and used exclusively by staff).
— To buy food for the stray cats at the hospital, as these animals can provide the best therapy for patients — millions of times better than wasting money poisoning and sedating them with drugs.
— To refurbish the hospital properly, rather than closing one ward after another for work that is either never finished or takes years to complete.
— To equip the Occupational Therapy department with the necessary resources to provide activities that fill the patients' time.
— To inform patients of the frightening side effects of the psychiatric medications they are forced to swallow or are injected with.
— To educate them about their rights — specifically their right to prior consent as stipulated in the Mental Health Act — rather than imposing such poison on them without consent or warning of the side effects.
Finally, a truly independent commissioner should be appointed (certainly not someone from the sadistic mental health sector) to safeguard patients' rights. We should not be left with a fake hospital "customer care" office that exists only to immediately inform staff when a report is filed against them, providing them with inside information. Nor should we have a "fake" Commissioner for Mental Health who covers up the abuses of psychiatrists and assists in intimidating patients by issuing continuous treatment orders, detention orders, and "Restriction of Freedom of Communication" (ROFOCO) orders. Part of therapy is to listen to the patients, not to invalidate them. Instead, in Psychiatry, they do the exact opposite: they intentionally destroy you with drugs and break you psychologically through measures like ROFOCOs.
I appreciate your acknowledgement that it is an "established fact that choking may be a hazard in patients undergoing psychiatric medication." Subjecting a patient to psychiatric medication ends up making them sick with so many terrible side effects that it becomes an excuse to drug them further to combat those very same side effects — a big business for the pharmaceutical industry driven by the evils of Psychiatry. It is like giving a tetanus vaccine to your newborn, but doing it with an AIDS-contaminated needle.
I am fairly certain you also know that in Psychiatry, there is not the slightest scientific basis for their diagnoses. The stroke of a pen is all that is needed for one to find themselves maliciously labeled with the most absurd, invented-for-the-occasion mental illnesses — labels especially suited for "crime laundering" and covering up institutional wrongdoing.
In the emails I attached (a, b, link1, link2) when you asked me to whom I had reported that tragic incident, I highlighted more than enough abuses from my own case that surely cannot have gone unnoticed by you. But instead of being a catalyst for change, you opted to continue the cover-up of these abuses. By closing not one eye but both, you would rather see me kept innocently locked away, kidnapped, and abused at leisure than take steps that might incriminate the "big heads" — the ones who have long merited being behind bars.
Because my cries have always fallen on deaf ears, it is I who must spend yet another festive season locked away while the culprits run scot-free. Perhaps you have heard this phrase before: “It is not only what we do, but also what we do not do, for which we are accountable.' ”
Final Note on Psychiatrist Hector Cutajar: When I wrote this previous email — only months after fighting through endless obstacles to transfer to Consultant Psychiatrist Joseph Spiteri — fate decreed that instead of Mark Xuereb appearing on Spiteri’s behalf, they assigned Hector Cutajar. I remembered him as the "yes-man" to the sadistic David Cassar; as such, I feared my ordeal was starting all over again.
Initially, I blamed Cutajar entirely for the death of patient MA, who tragically choked on a piece of bread, hoping this would lead to him being replaced. However, looking back at that day (November 15, 2020), Cutajar arrived all out of breath, having rushed to the scene. He reached the patient while the nursing staff of Male Ward 7 were still standing idly by, pretending to contact emergency services — to the point that they hadn't even deployed the emergency trolley. All this occurred while MA lay breathless on the floor.
While the medical response could certainly have been handled better, the primary failure lay with the nursing staff. They were entirely passive, waiting for Cutajar to give them basic instructions for every move. Even more to blame was Marlene Grech (Nursing Officer of Male Ward 7). In her typical fashion, she arrived late — long after the crisis had peaked and there was nothing left to be done to save MA
Above image shows the LifeVac choking rescue device.
Staff Misconduct and Patient Neglect at Mount Carmel Hospital

The images above reveal a disturbing misuse of government resources and a blatant disregard for patient welfare. In the right image, Marlene Grech, the Nursing Officer (NO) and head of Male Ward 7, is seen in uniform with her kid. Below that is a close-up of the notice she affixed to the ward door:
"Very important: No relatives are to be allowed in the ward for any reason at all. Relatives are to sign for patients outside the ward door. Thank you."
While relatives were strictly barred from entry, the ward's management operated under a different set of rules. Male Ward 7 originally contained two single rooms intended for patients. However, due to overstaffing, these rooms were repurposed for staff use. One became a locker room, while the other was claimed by Marlene Grech as a private office — complete with a computer, internet, toilet, and shower — at the hospital’s expense.
A "Private Childcare" at Patients' Expense: Instead of using this office for administrative duties, it was abusively transformed into a private childcare space. Throughout the summer months, Grech’s kids spent their days playing inside (note the children in shorts).
The hypocrisy is staggering. While staff children moved freely through the ward, patients were treated like lepers, forced to receive visitors behind Perspex screens under the guise of COVID-19 safety measures. By bringing children into a clinical environment during the pandemic, Marlene irresponsibly risked the lives of vulnerable patients. Furthermore, this occupied space denied patients — who already face the heavy stigma of being labeled "mentals" — their right to privacy.
Retaliation and Systemic Corruption: In August 2022, I reported these abuses to CEO Stephanie Xuereb, but no action was taken. Shortly after two patients tested positive for COVID-19, Marlene began shouting at management, demanding that all patients be swabbed because "we [the staff] have families at home." Her concern was for her own family's safety, despite having spent the summer exposing the ward to outside risks.
The culture of abuse is contagious; even the ward secretary began bringing her child to play, following the NO's corrupt example. Instead of addressing these grievances, the authorities have consistently protected the staff and assisted them in retaliating against patients who dare to speak out.
The "Messa in Scena" and Psychological Torture: Marlene Grech and nurse Joe Galea take a sadistic approach to patient care, constantly seeking new ways to isolate us. On February 22, 2023, the Commissioner for Health (Ombudsman) Raymond Galea visited me in hospital to discuss my reports (a clear conflict of interest is evident, as he is listed here as serving on a medical board with the other psychiatrists in question). This meeting turned out to be a messa in scena (a staged performance).
The retaliation was swift:
— The same evening: Smartphones were banned in Male Ward 7 to further isolate patients.
— March 2, 2023: A "restriction of freedom of communication" order was imposed on me.
— March 16, 2023: I was transferred to Male Ward 1 to be further isolated and psychologically pressured.
In the field of psychiatry, the story is always the same: it is not those who abuse the patients who are punished, but rather the patients who have the audacity to report the abuse.
More from the dark reality of Mount Carmel Hospital

The sadistic nurse Joe Galea
The sight of nurse Joe Galea laughing heartily is unsettling; his moustache only further portrays the inherent evil he embodies. Although he is a PN lackey, he reminds me of the frightening days of my childhood under the regime of Prime Minister Dom Mintoff. Mintoff literally sold Malta to Gaddafi, whose supporters — the "Labourites" — frequently sported moustaches. These were the individuals blessed with cozy jobs, social benefits, and housing stolen from those less fortunate.
Under Mintoff, a multitude of Libyans were brought in under the guise of "tourists" to Arabize us, even making the Arabic language compulsory. I see a direct parallel here: just as Mintoff forced a foreign culture upon us, psychiatrists and nurses today dehumanize their victims by forcing them to swallow the "poison" of psychiatric pills and injections.
I believe Galea vents the frustration of seeing his party, the PN, become increasingly irrelevant after years in opposition on his patients. Ironically, he seems to find inspiration for this behavior in the never-ending injustices of the Mintoff era.
Mintoff may have died on a date of strange numerical significance to my family — it was my sister’s 49th (7 x 7) birthday, my 36th (6 x 6), and exactly 666 + 9 days after Magistrate Carol Peralta’s vindictive court sentence on June 26, 2014. It was also 25 (5 x 5) years since the 1987 election, the year my father’s life was spared; I was saved from becoming fatherless at age ten and from being forced to learn Arabic. Yet, Mintoff's evil lives on, manifesting now on a much larger scale within Psychiatry. Both systems may appear benevolent or well-intentioned at first, but their side effects are devastating.

Psychotherapist Elizabeth Abdilla
I have previously stated that the staff at Mount Carmel Hospital compete with psychiatrists in their sadism and abuse of patients; Elizabeth Abdilla is a prime example. She is abusively absent, spending more time on sick leave than at work. The doctors who fraudulently issue her multitude of sick leave certificates merit a full investigation, especially since she appears healthy enough to pursue her Criminology course at the University of Malta (a fact she proudly displays on ResearchGate) while "sick".
On Monday, February 27, 2023, a few days after the staff in Male Ward 7 (MW7) confiscated my mobile phone, I requested her assistance through the Occupational Therapy department. For the second time, I made her fully aware of the abuses I was enduring. I urged her to consult this website for evidence wherever she had doubts, hoping she would put her studies as a "criminologist" into practice.
Not only was she useless as a psychotherapist, but she actively furthered the staff's agenda. She assisted in their revenge against me, leading to yet another restriction of communication order on March 2, 2023. This culminated in my expulsion from MW7 to MW1 on March 16, 2023.
It is clear she views her former Dean, the sadistic Andrew Azzopardi, as a role model and inspiration. By following his example, she incriminates herself as a fraud — the same brand of "fake criminologist" that Roberta Holland taught her to be.
One of the most negligent figures I encountered during my time at Mount Carmel Hospital was Nurse Joe Galea. His tenure was marked by a chilling lack of empathy and a series of incidents that still haunt those of us who were under his "care."
Negligence and Tragedy: Galea was on duty for half-day overtime during the tragic events of Sunday, November 15, 2020, when a patient choked on his food. The staff present proved completely incompetent, failing to save the man’s life. Galea then returned for his night shift and spent almost the entire time asleep, totally unbothered by the morning's tragedy. Similarly negligent was Nursing Officer Marlene Grech, who arrived — as was her norm — nearly an hour late, turning up only when there was nothing left to save.
The COVID-19 Transfer: The mistreatment didn't stop at negligence; it extended to a systematic stripping of our basic rights and dignity. In March 2021, fifteen of us were transferred to another ward for a fortnight after testing positive for COVID-19. We were strictly ordered to leave all our belongings behind. When we returned, far from being welcomed back, we found that our personal lockers had been smashed open. Several patients reported belongings missing; I found my own mobile phone with a cracked screen. When I reported that my locker had been broken into, Galea played the fool, acting as if he knew nothing when asked to contact maintenance to repair the lock.
Systemic Abuse and Petty Tyranny: When I asked for a mirror to shave my two-week-old beard and a place to plug in my charger, Galea began grumbling: “Għadhom kif ġew, ġa bdew iridu l-mera, biex iqabbdu ċ-charger” (They just got back and already they want the mirror and the charger).
Accessing basic hygiene became a psychological battle. When I needed a mirror to shave, I often delayed it for days, waiting until Galea or the other negligent staff were out of the office. Asking for a simple mirror felt like an impossible task for them to handle for a "miserable patient."
Calculated Control: The lockers were originally elevated on platforms (as seen in this image, where my broken laptop is resting). Galea eventually had these platforms dismantled one by one. His excuse was that patients were using them to nap during the day. In reality, it was a calculated move to ensure we were exhausted by nighttime, preventing anyone from walking around and disturbing his ability to sleep through his night shifts. One particular nurse from Gozo, similar to Marlene Grech, consistently arrived an hour late and left an hour early during day shifts. However, on night shifts, he often remained asleep an hour after his shift was supposed to have ended.
Galea reduced the number of lockers available to patients by half, seizing some for staff use — a move that felt like state-sponsored theft — and dumping others. He rearranged the remaining lockers to create yet another staff room, bringing their total to five dedicated staff areas, plus a store used as a spare bedroom.
Environmental Sabotage: Galea’s priority was always his own comfort, specifically his sleep. He moved a set of eleven chairs away from the clinic area because the sound of patients chatting annoyed him. He even had the aluminum door removed from one of the two patient toilet cubicles just to reduce the noise of doors opening and closing during the night.
Similarly, because the smoking room door bothered him, he ensured a padlock was placed on it to keep it shut all night. This forced patients to smoke in the toilets and dormitories. After eight years of being symptom-free, the resulting poor air quality triggered a return of my asthma attacks. Previously, he would even confiscate cigarette lighters during night shifts, all to ensure that "cursed door" wouldn't wake him from his sleep.
His hypocrisy was constant. He had a habit of peeing in and dirtying the patients' toilets, yet when he needed to relieve himself, he retreated to the clean staff toilets reserved strictly for their own use.
The Case of Patient GA: In June 2022, a patient my age, GA, returned to the ward. He suffered from chronic pain — likely a side effect of the Risperdal he was prescribed — which kept him awake. When he asked for Panadol at midnight, he accidentally woke Galea. In retaliation, Galea conspired with Nursing Officer Marlene Grech to have him transferred.
They found their excuse when GA returned from an appointment at Mater Dei Hospital. He had stopped at a vending machine to buy cigarettes with a small amount of pocket money from his parents. Using the petty excuse that he shouldn't have had cash, they had him transferred to the Maximum Secure Unit (MSU), where he remained for several months as punishment for "interrupting" a nurse's sleep.
Malpractice and Retaliation: Around December 2022, a patient named JR was admitted to Male Ward 7. Perhaps due to an intellectual disability, he spent much of his time laughing to himself or inadvertently annoying others; he often remained awake throughout the night. When Nurse Joe Galea was assigned the night shift, something changed. Unlike other nights, about an hour after JR was given his evening medication, he became so heavily sedated that he had to be dragged to bed. By morning, he was found soaked in his own urine and remained confined to a wheelchair until evening, unable to stand.
The morning staff didn't bother calling a doctor. Suspicion grew among the patients that Galea — well known for his lack of ethics — had administered extra medication to ensure JR slept through the night. The police were eventually contacted. The following night, another negligent nurse began threatening us, vowing revenge on whoever had reported the incident. After he administered JR’s pills that night, the patient again became so dangerously unresponsive that he had to be rushed to Mater Dei Hospital.
Silencing the Voiceless: Psychiatry, at its core, often feels structured to facilitate cover-ups; those who report abuse are tracked and punished, while perpetrators remain protected. Infuriated that anyone would dare expose their conduct, the staff began pushing for a ban on smartphones in the wards. Their goal was clear: to eliminate any means of documenting abuse and ensure we remained intimidated and silenced. The final straw for the staff was a visit from the Commissioner for Health within the Ombudsman's office, Raymond Galea, on February 22, 2023. Far from being helpful, the visit felt like a premeditated, staged act.
Exploitation and Theft: The exploitation was even petty. The same nurse frequently brought cooked rice or pasta to sell to patients during night shifts. Furthermore, when we patients made biscuits during occupational therapy, some staff would often take the majority home or eat them themselves. The meager leftovers were intentionally distributed only when most patients were out in the main garden, ensuring very few of us received what we had actually worked to create.
One can only imagine how many sadistic abuses patients must endure for the staff to persevere in their cruelty so endlessly, with ever-greater intensity and impunity. If only we could use their own twisted logic against them — to label them as "unable to realize the severity of their actions" and have them drugged or injected with the same psychiatric poisons they use on patients for the slightest mishap. If only they could taste their own medicine.
Of course, there are a few staff members who are exceptional, or at least do not go to such horrific extremes, but they are the very, very few.
The Cost of Corruption: How Taxpayer Money is Being Drained
Socialism, in its current local iteration, is failing us. Historically, supporters of past Labour governments sought "cushy" government jobs or fraudulent medical boarding. However, under the current administration, the situation has escalated. We now see a system where contractors and speculators pressure ministers to import foreign labor, solely so these workers can funnel their wages back to landlords as rent.
The Privatization of Mental Healthcare: The systematic dismantling of Mount Carmel Hospital is a prime example of "Corrupt-Malta-Style" politics. Wards are being closed or demolished one after another, creating a convenient excuse to outsource patients to private nursing homes — all, most probably, in exchange for party donations.
Dysfunction in the Wards: The video above captures the "hard work" taking place in Male Ward 7. While the entire facility struggles, this ward — managed by an individual notorious for her own abuses — is particularly egregious. Taxpayers are essentially paying the middleman the salary of a doctor or nurse for the services of a carer who often has nothing to do. We are indirectly subsidizing a cycle that benefits the construction industry:
- Mass Migration: Higher demand leads to skyrocketing rents and property prices, further fueling the destruction of Malta’s landscape with the "ugly" apartment blocks ruining the island.
- Strained Infrastructure: After paying minimal tax for just a few months, foreign workers qualify for free healthcare, transport, and education for their many children, alongside various social benefits.
- The Wage Gap: While such staff earn double or triple pay for Sundays and public holidays while doing very little, many pensioners struggle to survive until the end of the month.
A Culture of Fraud: The lack of accountability is staggering. In the video, staff are seen chatting, playing on their phones, or even sleeping — to the point that their salary is effectively just another form of social benefit. If this is the behavior during the day, one can only imagine the state of the night shifts.
The issue is bolstered by a refusal to implement modern attendance tracking. The August 2023 sectoral agreement (supported by 87% of nurses) stipulated that electronic palm readers would only be used if applied to all employees, regardless of grade. This is a deliberate "poison pill" because high-level officials and psychiatrists will likely never agree to it.
This lack of oversight allowed for scandals like that of MUMN President Paul Pace. He was caught claiming thousands in overtime for hours he never worked at Mount Carmel Hospital — even while he was on holiday in Egypt. When "work" and "vacation" look identical because no actual labor is being performed, the country’s public debt will continue to spiral until we face inevitable bankruptcy.
Systemic Abuse and the Silencing of Patients: Rest assured, if proper time-logging were implemented, many of these staff members wouldn't total more than 30 minutes of actual work in a 12-hour shift; the rest do nothing at all. Deep down, they know they are being paid for doing nothing. This creates a toxic environment where staff suffer from a "guilty conscience" or an obsessive fear of being reported. To protect their "cushy" jobs, they look for any excuse to make patients even more voiceless, allowing them to continue their abuses with total peace of mind.
This is a direct violation of the Mental Health Act, Article 3.1.r, which beautifully states that a patient should have the right to "free and unrestricted communication with the outside world." In practice, the opposite occurs. They have prohibited patients from using mobile phones to further silence them, leaving them with nothing to do but descend into further distress.
Impunity and Retaliation: Patients are reported for the slightest mishap. If you dare to confront the staff, they instantly shut you down with labels meant to discredit you:
- "Ġie paranojd għall-istaff" (Became paranoid toward the staff)
- "Imħawwad" (Confused/Disoriented)
- "Imtektek" (Unstable)
- "Escalation of behavior"
While patients are labeled and silenced, the staff abuses their positions in broad daylight with total impunity and the blessing of the authorities. It is a case where psychiatry never fails to cross the limits of decency.
As a recent article summed it up: "MUMN boss [Paul Pace] abuses his position for personal gain" — a fact admitted by the Mount Carmel CEO herself. Yet, when action is threatened against corrupt figures like this, the response is often that they will use their position to retaliate by issuing directives that negatively affect the service.
Essentially, the message from the top is: Let them enjoy impunity galore, and to hell with the miserable patients. If a single corrupt official can blackmail the CEO so easily, one can only imagine the revenge the staff takes on patients — myself being a prime example — who dare to speak out and report them.
The Architecture of Fraud: From Medical Boards to Criminal Benefits
The corruption extends to the very top. Consider Psychiatrist Joseph Spiteri, the Deputy Chairman of Psychiatry. Together with Psychiatrist Hector Cutajar, he issued me my fourth Restriction of Freedom of Communication Order (ROFOCO), along with many subsequent orders.

Evidence shows that Spiteri’s professional conduct is defined by the "stroke of a pen" for the right price. Allegations have surfaced that prisoners pay sums of money to be fraudulently "boarded out." For a fee, he diagnoses them with non-existent mental illnesses — diagnoses that, as is typical in psychiatry, lack any scientific basis — leaving taxpayers to foot the bill.
A Prophecy of Corruption: It is worth noting that I attempted to expose this long ago. On June 29, 2023 — months before the general benefits scandal broke — I reached out to the newly appointed Ombudsman Joseph Zammit McKeon, the Social Security Compliance Unit, the Police, the Minister for Social Policy, and even the Times of Malta. I asked them all to investigate the fraudulent actions of Joseph Spiteri. My warnings were met with silence, proving the depth of the protection these figures enjoy.
The Disability Benefits Scandal: Spiteri is also linked to others — including psychiatrist Hector Cutajar, Doreen Cassar (wife of Psychiatrist David Cassar), and Raymond Galea (the recently appointed Commissioner of Health within the Ombudsman) — who formed the Medical Board responsible for approving social benefits. This board was recently embroiled in a massive disability benefits fraud scandal. Witnesses stated that:
- Interviews often lasted a mere five minutes.
- Weeks later, individuals began receiving monthly payments of approximately €450.
Many of these beneficiaries possibly were criminals or who had never paid a cent in tax, yet were granted benefits with ease.
Selective "Disability": The Case Against Me: There is a glaring double standard at play. While Spiteri and his associates facilitate benefits for criminals, they have never extended such "generosity" to me. Despite being maliciously labeled with "chronic and severe" mental illnesses for years, I have been denied similar support.
The reason is simple: I refuse the label. I have gathered evidence of the massive fraud behind these diagnoses. While criminals work hand-in-hand with psychiatrists to exploit the system, I have been targeted with ten consecutive ROFOCOs because I dared to unmask them.
Silencing the Truth: In the twisted logic of local psychiatry, the abuser is never wrong; the one who reports the abuse is the problem. They cannot stand the truth or the evidence presented on this website.
The proof that my claims hit the mark is in their reaction. If I were spreading lies or exaggerations, they wouldn't need to issue communication bans (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12). Instead, they would have flooded the media with statements labeling this site as "misleading" — much like the fear-mongering campaigns seen during the COVID-19 era. Their silence, enforced through abusive restrictions on my right to speak, is their only defense against the truth.
The "Greatest Fraudsters and Crime-Launderers"
 The super mega fraudster (1, 2, {3}, 4, 5, 6, 7, 8, 9, "Tell me you are sick ...", etc.) and sadistic (4, 5,
6,
7,
8,
9,
10, 11, 12, skin alive) and extremely vulgar (chop off / all: a, b, c, d) Psychiatrist Joseph Spiteri
The super mega fraudster (1, 2, {3}, 4, 5, 6, 7, 8, 9, "Tell me you are sick ...", etc.) and sadistic (4, 5,
6,
7,
8,
9,
10, 11, 12, skin alive) and extremely vulgar (chop off / all: a, b, c, d) Psychiatrist Joseph Spiteri Psychiatrist Joseph Saliba
Psychiatrist Joseph Saliba Professur tal-bigilla Psychiatrist David Mamo
Professur tal-bigilla Psychiatrist David MamoThese individuals merit the title of the greatest fraudsters of our time. On May 2 and May 16, 2023, I was examined by these psychiatrists. On June 6, they also spoke with my sisters. Together, we made them fully aware — more than they already were — of the abuses I have suffered. We clarified and elaborated on the evidence presented on this website, which Spiteri had printed out, seemingly as an attempt to intimidate me.
The Myth of "Mental Immunity": A telling moment occurred when my sister asked why, unlike journalist Daphne Caruana Galizia who faced over 40 libel cases, I have faced none despite the gravity of my claims. The hypocritical response from Spiteri was that it is because I am "still considered a mental."
Apparently, beyond parliamentary immunity, there exists "mental immunity." This is a convenient fiction. Consider Magistrate Peralta, who once had a journalist arrested and called "parasite scum"; does anyone truly believe he would tolerate a "mental" patient writing truthfully or otherwise about him on this website if the law actually allowed him to stop it? They use the "mental" label not to protect me, but to avoid the legal discovery that a court case would bring.
Academic and Administrative Rot — The corruption extends through the entire hierarchy:
- Psychiatrist David Mamo: He is the ultimate example of a Professur tal-bigilla (a sham professor), precisely what one expects from a university in a corrupt state — specifically within the Faculty of Social Wellbeing, where former Dean Andrew Azzopardi issues "fatwas" under the guise of social wellbeing.
- Psychiatrist Joseph Saliba: In his heyday as Superintendent of Psychiatry, he wielded immense power. Evidence in these emails shows he was sent by the former Commissioner for Mental Health, John Cachia, to cover up staff abuses I reported in 2018 — specifically, staff stealing hospital food intended for patients.
A Failed Science: If these "professionals" will cover up petty theft, they will certainly cover up the sadistic abuses of their colleagues. These psychiatrists are, in my view, nothing more than failed doctors and state-sponsored drug pushers. Because they have no real science to back their claims, they vent their frustrations by transforming into the most sadistic hypocrites imaginable. They operate with a total disregard for their victims, prioritizing the protection of their own fraudulent system above all else.
Media Confirmation: Systematic Theft and "Double-Dipping"
 On December 22, 2023, The Shift News published an article titled Systematic Abuse and Theft in Overtime, Allowances at Mt Carmel Hospital. The report revealed that some medical consultants — the very psychiatrists I have been exposing — were being paid allowances that surpassed their basic pay by up to 200%.
On December 22, 2023, The Shift News published an article titled Systematic Abuse and Theft in Overtime, Allowances at Mt Carmel Hospital. The report revealed that some medical consultants — the very psychiatrists I have been exposing — were being paid allowances that surpassed their basic pay by up to 200%.
Days later, on December 28, 2023, the parrots at Times of Malta followed suit, reporting that staff were found working extra jobs during their official hospital hours. In one instance, an audit found a consultant being paid by the Commissioner for Mental Health while simultaneously on the clock at Mount Carmel. This same consultant was also working for the Court Services Agency and the Malta Foundation School.
Notably, while the local media was quick to name MUMN President Paul Pace, they protected these consultants by keeping their identities anonymous.
Warnings Ignored — The 2020 Emails: What makes this "discovery" by the media so incredible is that I had already highlighted these exact abuses to CEO Stephanie Xuereb over three and a half years earlier. In an email dated June 12, 2020, I wrote:
"The staff abuse the system intentionally because they see that those above them — the doctors and psychiatrists — do the same or worse. Many of these consultants hold multiple jobs: private clinics, court experts, university lecturers, and TV appearances. Ask yourself how they find time for all of this, plus a family, while supposedly working a full-time hospital job.
While they are on the clock at the hospital, they are performing outside work for separate pay — preparing court reports, lectures, or TV segments like Anton Grech. If you claim not to know this, you must be living on the moon. For my own court report, David Cassar and Ethel Felice conducted their evaluation during the hours they were supposed to be working their full-time hospital jobs. They were being paid from two sources at the same time."
Retaliation and Sabotage: Instead of taking action against this fraud, CEO Stephanie Xuereb — a master fraudster and sadist — orchestrated a campaign of revenge against me. Within a week of my report:
- I was transferred to a ward with "savage" conditions.
- I was placed on Level 1 supervision, with staff watching me 24 hours a day.
- A one-month ROFOCO (Restriction of Freedom of Communication Order) was issued on June 19, 2020, followed by another on August 14, 2020, to silence me.
To further intimidate me, my laptop — which had been held in the hospital safe during the communication ban — was returned to me with a smashed screen. After the CEO initially lied and denied any negligence, the hospital eventually issued a measly €140 refund for the repairs more than a year and a half later. This was a clear attempt to break my spirit, silence my evidence, and allow their culture of impunity to continue unhindered.
 The image above shows a Continuous Detention Order. With a single stroke of a pen, a patient is locked away by sadistic psychiatrists for a staggering six months.
The image above shows a Continuous Detention Order. With a single stroke of a pen, a patient is locked away by sadistic psychiatrists for a staggering six months.
When this patient could no longer endure being innocently confined, over-medicated without cause, and watching his health deteriorate from the blatant side effects of psychiatric drugs, he escaped from Mount Carmel Hospital. It was the animal instinct for survival — the drive to fight for your rights and stay "busy living" — to prove to the outside world that he could function perfectly well without their "cure."
As an act of collective punishment, the staff of MW7 then locked the remaining patients inside the ward 24/7, stripping away even the briefest access to the yard for fresh air. This draws a chilling parallel to the atrocities of World War II: when a prisoner escaped, the guards would murder ten remaining prisoners in revenge.
In corrupt Malta, such orders are not the exception; they are the norm. In Maltese, we say: "qishom qed ibighu l-pastizzi" (as if they are selling cheesecakes). With a "Commissioner for Mental Health" who serves as nothing more than a rubber stamp for whatever the psychiatrists dictate, psychiatry has found fertile ground to abuse human rights at leisure. This is the true, diabolic face of the system.
The video above, filmed by a resident on a smartphone at the St. Vincent de Paul home for the elderly, captures a carer mishandling a vulnerable senior. Now, try to imagine the abuses — not only physical but verbal — that occur a billion times more severely at Mount Carmel Hospital. In Mount Carmel, patients are easily discredited, framed, and stigmatized.
Anything a patient says is taken with a pinch of salt; if they dare to speak out, they are labeled as "delusional" or accused of having "inappropriate beliefs." They are drugged as a form of retaliation. I have even seen staff damage patients' personal belongings — my own laptop and mobile included — out of pure spite.
By denying patients the use of smartphones in the wards, the administration ensures they remain voiceless. This allows the staff to abuse their power at leisure, confident that no one will believe the victims. They act with the full knowledge that the authorities are always ready to cover up even their most sadistic acts against the vulnerable.
 In corrupt Malta, psychiatrists have sought the services of freelance writers like Belle de Jong to pen stories and articles promoting their agenda. Their hidden goal? To see Mount Carmel Hospital closed and relocated to a new facility next to Mater Dei. It is truly incredible. So much of psychiatry is a facade; our local media are merely puppets on a string, and money is the only thing that speaks.
In corrupt Malta, psychiatrists have sought the services of freelance writers like Belle de Jong to pen stories and articles promoting their agenda. Their hidden goal? To see Mount Carmel Hospital closed and relocated to a new facility next to Mater Dei. It is truly incredible. So much of psychiatry is a facade; our local media are merely puppets on a string, and money is the only thing that speaks.
In reality, if a patient writes to the media to expose the truth, their letters are ignored — as happened to me and many others. This aggressive lobbying to build a new hospital is causing immense mental stress for both patients and staff. A new building will solve nothing regarding stigma; within a short time, it will simply become known as the "New Ta' Frankuni," and we will be back to square one.
The only ones who stand to gain are the psychiatrists, who wish to pride themselves on having a facility next to Mater Dei just to appear as "real" doctors — all at the taxpayer's expense. When someone like Belle calls herself a "Mental Health Advocate" while simultaneously participating in my character assassination — labeling me a "cat killer" despite evidence to the contrary — she is giving the public a small taste of the far worse abuses one can expect from the evil of psychiatry.